

Zinc for the prevention or treatment of acute viral respiratory tract infections in adults: a rapid systematic review and meta-analysis of randomised controlled trials
- PMID: 34728441
- PMCID: PMC8578211
- DOI: 10.1136/bmjopen-2020-047474
Zinc for the prevention or treatment of acute viral respiratory tract infections in adults: a rapid systematic review and meta-analysis of randomised controlled trials
Abstract
Objective: To evaluate the benefits and risks of zinc formulations compared with controls for prevention or treatment of acute viral respiratory tract infections (RTIs) in adults.
Method: Seventeen English and Chinese databases were searched in April/May 2020 for randomised controlled trials (RCTs), and from April/May 2020 to August 2020 for SARS-CoV-2 RCTs. Cochrane rapid review methods were applied. Quality appraisals used the Risk of Bias 2.0 and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
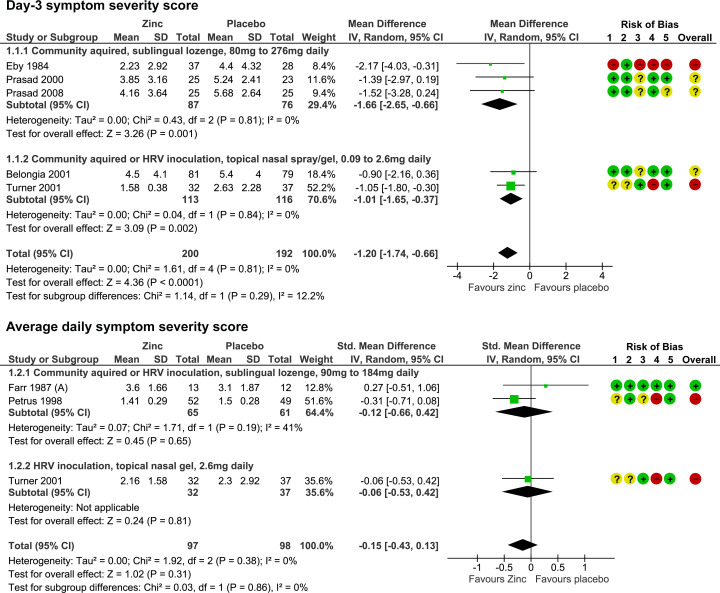
Results: Twenty-eight RCTs with 5446 participants were identified. None were specific to SARS-CoV-2. Compared with placebo, oral or intranasal zinc prevented 5 RTIs per 100 person-months (95% CI 1 to 8, numbers needed to treat (NNT)=20, moderate-certainty/quality). Sublingual zinc did not prevent clinical colds following human rhinovirus inoculations (relative risk, RR 0.96, 95% CI 0.77 to 1.21, moderate-certainty/quality). On average, symptoms resolved 2 days earlier with sublingual or intranasal zinc compared with placebo (95% CI 0.61 to 3.50, very low-certainty/quality) and 19 more adults per 100 were likely to remain symptomatic on day 7 without zinc (95% CI 2 to 38, NNT=5, low-certainty/quality). There were clinically significant reductions in day 3 symptom severity scores (mean difference, MD -1.20 points, 95% CI -0.66 to -1.74, low-certainty/quality), but not average daily symptom severity scores (standardised MD -0.15, 95% CI -0.43 to 0.13, low-certainty/quality). Non-serious adverse events (AEs) (eg, nausea, mouth/nasal irritation) were higher (RR 1.41, 95% CI 1.17 to 1.69, NNHarm=7, moderate-certainty/quality). Compared with active controls, there were no differences in illness duration or AEs (low-certainty/quality). No serious AEs were reported in the 25 RCTs that monitored them (low-certainty/quality).
Conclusions: In adult populations unlikely to be zinc deficient, there was some evidence suggesting zinc might prevent RTIs symptoms and shorten duration. Non-serious AEs may limit tolerability for some. The comparative efficacy/effectiveness of different zinc formulations and doses were unclear. The GRADE-certainty/quality of the evidence was limited by a high risk of bias, small sample sizes and/or heterogeneity. Further research, including SARS-CoV-2 clinical trials is warranted.
Prospero registration number: CRD42020182044.
Keywords: complementary medicine; nutrition & dietetics; respiratory infections; therapeutics.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form (available on request from the corresponding author) and declare: no support from any organisation for the submitted work. DM and SL have no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work. SA, JH and GY are academic researchers at NICM Health Research Institute. As a medical research institute, NICM Health Research Institute receives research grants and donations from foundations, universities, government agencies, individuals and industry. Sponsors and donors provide untied funding for work to advance the vision and mission of the Institute. This review was not undertaken as part of a contractual relationship with any donor or sponsor. JH is an academic general practitioner with a clinical interest in integrative medicine, has received payment for providing expert advice about traditional, complementary and integrative medicine, including nutraceuticals, to industry, government bodies and non-government organisations, and spoken at workshops, seminars and conferences for which registration, travel and/or accommodation has been paid for by the organisers. SA is a naturopathic practitioner at an obstetrics and gynaecology clinic in Sydney, Australia. She has received payment for providing expert editing of naturopathic and herbal medicine educational programmes, and for investigation of naturopathy, herbal medicines and nutraceuticals in clinical trials and spoken at workshops, seminars and conferences for which registration, travel and/or accommodation has been paid by the organisers. GY is an academic researcher with interest in complementary and integrative medicine. She has spoken at research workshops, seminars and conferences for which registration and travel has been paid by the organisers. JG is a naturopathic doctor and director of a functional bowel disease clinic in Colorado Springs, USA. JG has spoken at research conferences for which registration, travel and/or accommodation has been paid by the organisers. He is also a research investigator at the Helfgott Research Institute, National University of Natural Medicine. As a medical research institute, Helfgott receives research grants and untied donations from foundations, universities, government agencies, individuals, and industry. This review was not undertaken as part of a contractual relationship with any donor or sponsor. JB is an independent librarian and reports personal fees from Helfgott Research Institute, National University of Natural Medicine, during the conduct of the study. SPM is an academic researcher at Southern Cross University where he is a Professor of Traditional, Complementary and Integrative Medicine. SPM has received payment for providing expert advice to industry, government bodies and non-government organisations, and spoken at workshops, seminars and conferences for which registration, travel and/or accommodation has been paid for by the organisers. This review was not undertaken as part of a contractual relationship with any donor or sponsor.
Figures




References
-
- Avendaño Carvajal L, Perret Pérez C. Epidemiology of respiratory infections. Pediatric Respiratory Diseases 2020:263–72. 10.1007/978-3-030-26961-6_28 - DOI
-
- Eccles R, Weber O. Common cold. Secaucus: Birkhäuser, 2009.
-
- CDC . Antibiotic prescribing and use in doctor’s offices: adults treatment recommendations, 2017. Centres for disease control and prevention. Available: https://www.cdc.gov/antibiotic-use/index.html [Accessed 4 Oct 2020].
-
- Gruffydd-Jones K, Hickman K. Managing dilemmas in respiratory infections and antibiotic prescribing. Primary Care Respiratory update 2018;5:32–5 https://www.pcrs-uk.org/sites/pcrs-uk.org/files/RTI_Antbx_5_1_2018.pdf
-
- DeGeorge KC, Ring DJ, Dalrymple SN. Treatment of the common cold. Am Fam Physician 2019;100:281–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous