

Defining hypoxaemia from pulse oximeter measurements of oxygen saturation in well children at low altitude in Bangladesh: an observational study
- PMID: 34728475
- PMCID: PMC8565559
- DOI: 10.1136/bmjresp-2021-001023
Defining hypoxaemia from pulse oximeter measurements of oxygen saturation in well children at low altitude in Bangladesh: an observational study
Abstract
Background: WHO defines hypoxaemia, a low peripheral arterial oxyhaemoglobin saturation (SpO2), as <90%. Although hypoxaemia is an important risk factor for mortality of children with respiratory infections, the optimal SpO2 threshold for defining hypoxaemia is uncertain in low-income and middle-income countries (LMICs). We derived a SpO2 threshold for hypoxaemia from well children in Bangladesh residing at low altitude.
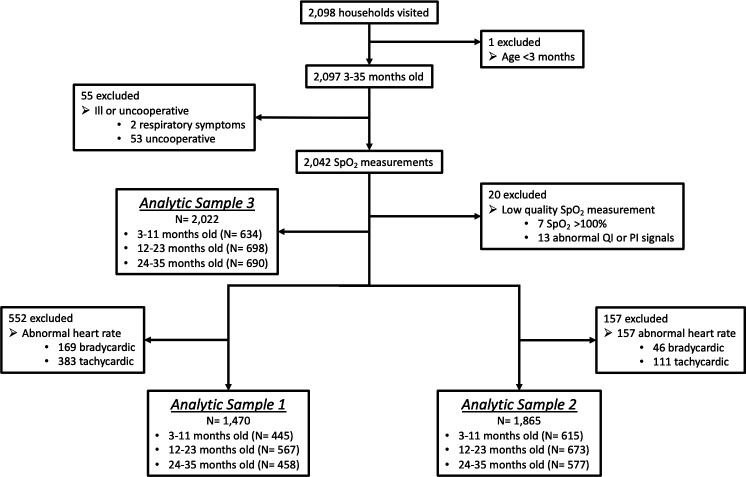
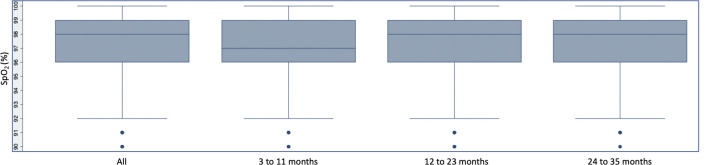
Methods: We prospectively enrolled well, children aged 3-35 months participating in a pneumococcal vaccine evaluation in Sylhet district, Bangladesh between June and August 2017. Trained health workers conducting community surveillance measured the SpO2 of children using a Masimo Rad-5 pulse oximeter with a wrap sensor. We used standard summary statistics to evaluate the SpO2 distribution, including whether the distribution differed by age or sex. We considered the 2.5th, 5th and 10th percentiles of SpO2 as possible lower thresholds for hypoxaemia.
Results: Our primary analytical sample included 1470 children (mean age 18.6±9.5 months). Median SpO2 was 98% (IQR 96%-99%), and the 2.5th, 5th and 10th percentile SpO2 was 91%, 92% and 94%. No child had a SpO2 <90%. Children 3-11 months had a lower median SpO2 (97%) than 12-23 months (98%) and 24-35 months (98%) (p=0.039). The SpO2 distribution did not differ by sex (p=0.959).
Conclusion: A SpO2 threshold for hypoxaemia derived from the 2.5th, 5th or 10th percentile of well children is higher than <90%. If a higher threshold than <90% is adopted into LMIC care algorithms then decision-making using SpO2 must also consider the child's clinical status to minimise misclassification of well children as hypoxaemic. Younger children in lower altitude LMICs may require a different threshold for hypoxaemia than older children. Evaluating the mortality risk of sick children using higher SpO2 thresholds for hypoxaemia is a key next step.
Keywords: paediatric lung disaese; pneumonia; respiratory infection.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- GBD 2017 Lower Respiratory Infections Collaborators . Quantifying risks and interventions that have affected the burden of lower respiratory infections among children younger than 5 years: an analysis for the global burden of disease study 2017. Lancet Infect Dis 2020;20:60–79. 10.1016/S1473-3099(19)30410-4 - DOI - PMC - PubMed
-
- World Health Organization . Integrated management of childhood illness: chart booklet. Geneva, Switzerland: World Health Organization, 2014. https://apps.who.int/iris/bitstream/handle/10665/104772/9789241506823_Ch...
-
- World Health Organization, . Pocketbook of hospital care for children. guidelines for the management of common childhood illnesses. second edition. 2nd edn. Geneva, Switzerland: World Health Organization, 2013. https://apps.who.int/iris/bitstream/handle/10665/81170/9789241548373_eng...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources