

Patients' perspectives of prehabilitation as an extension of Enhanced Recovery After Surgery protocols
- PMID: 34728523
- PMCID: PMC8565881
- DOI: 10.1503/cjs.014420
Patients' perspectives of prehabilitation as an extension of Enhanced Recovery After Surgery protocols
Erratum in
-
Correction: Patients’ perspectives of prehabilitation as an extension of Enhanced Recovery After Surgery protocols.Can J Surg. 2021 Nov 18;64(6):E620. doi: 10.1503/cjs.019521. Print 2021 Nov-Dec. Can J Surg. 2021. PMID: 34794971 Free PMC article. French. No abstract available.
Abstract
Background: Enhanced Recovery After Surgery (ERAS) and prehabilitation programs are evidence-based and patient-focused, yet meaningful patient input could further enhance these interventions to produce superior patient outcomes and patient experiences. We conducted a qualitative study with patients who had undergone colorectal surgery under ERAS care to determine how they prepared for surgery, their views on prehabilitation and how prehabilitation could be delivered to best meet patient needs.
Methods: We conducted semistructured interviews with adult patients who had undergone colorectal surgery under ERAS care within 3 months after surgery. Patients were enrolled between April 2018 and June 2019 through purposive sampling from 1 hospital in Alberta. The interview transcripts were analyzed independently by a researcher and a trained patient-researcher using inductive thematic analysis.
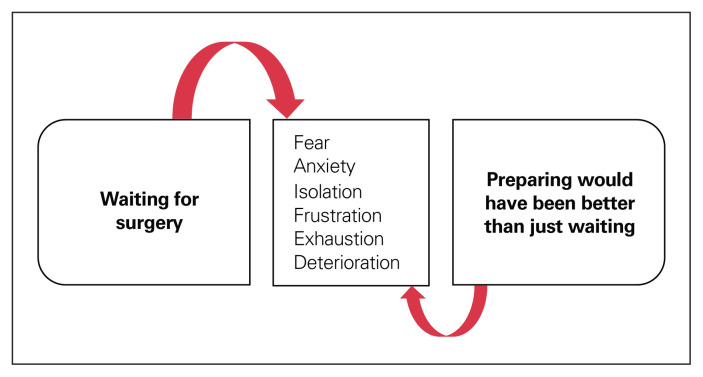
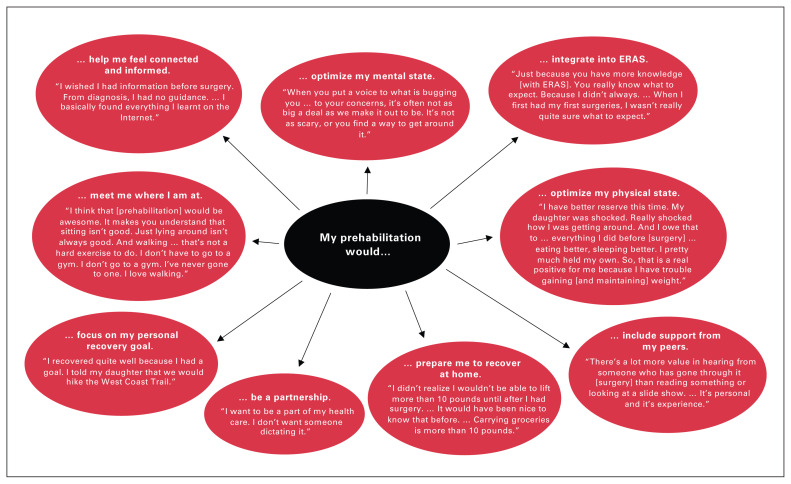
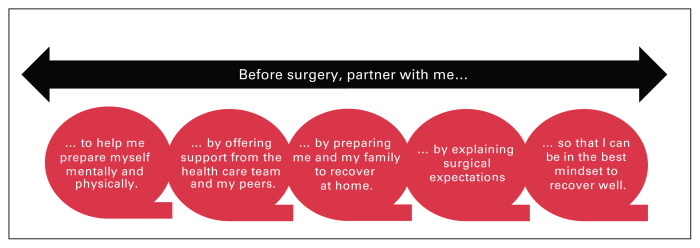
Results: Twenty patients were interviewed. Three main themes were identified. First, waiting for surgery: patients described fear, anxiety, isolation and deterioration of their mental and physical states as they waited passively for surgery. Second, preparing would have been better than just waiting: patients perceived that a prehabilitation program could prepare them for their operation if it addressed their emotional and physical needs, provided personalized support, offered home strategies, involved family and included surgical expectations (both what to expect and what is expected of them). Third, partnering with patients: preoperative preparation should occur on a continuum that meets patients where they are at and in a partnership that respects patients' expertise and desired level of engagement.
Conclusion: We identified several patient priorities for the preoperative period. Integrating these priorities within ERAS and prehabilitative programs could improve patient satisfaction, experiences and outcomes. Actively engaging patients in their care might alleviate some of the anxiety and fear associated with waiting passively for surgery.
Contexte:: Les protocoles de récupération optimisée après une chirurgie (ERAS, pour Enhanced Recovery After Surgery) et les programmes de préadaptation se fondent sur des données probantes et sont centrés sur les patients et pourtant, une plus grande contribution de ces derniers permettrait d’améliorer ces interventions et donneraient lieu à des résultats et des expériences plus satisfaisants pour les patients. Nous avons procédé à une étude qualitative auprès de patients ayant subi une chirurgie colorectale avec protocole ERAS afin de savoir comment ils se sont préparés à la chirurgie, quel est leur point de vue sur la préadaptation et en quoi cette dernière pourrait mieux répondre à leurs besoins.
Méthodes:: Nous avons réalisé des entrevues semi-structurées auprès de patients adultes ayant subi une chirurgie colorectale avec protocole ERAS dans les 3 mois suivant leur chirurgie. Les patients ont été inscrits dans un hôpital albertain entre avril 2018 et juin 2019 par le biais d’un échantillonnage dirigé. Les transcriptions des entrevues ont fait l’objet d’une analyse thématique inductive indépendante par une chercheuse et une patientechercheuse dûment formée.
Résultats:: Vingt patients ont été interrogés. Trois grands thèmes ont été dégagés : 1) en attente de la chirurgie (les patients ont fait état de peur, d’anxiété, d’un sentiment d’isolement et d’une détérioration de leur état de santé mentale et physique durant l’attente passive de la chirurgie); 2) une préparation leur a semblé préférable à une simple attente (les patients ont senti qu’un programme de préadaptation les aiderait à se préparer à leur chirurgie s’il tenait compte de leurs besoins émotionnels et physiques, s’il fournissait un soutien personnalisé, des stratégies de soutien à domicile, s’il impliquait les familles et incluait une discussion sur les attentes vis-à-vis de la chirurgie); et 3) partenariat avec les patients (la préparation devrait se dérouler selon un continuum adapté à la situation de chaque patient sous la forme d’un partenariat qui respecte son expertise et son niveau d’engagement).
Conclusion:: Nous avons identifié plusieurs priorités pour les patients durant l’étape préopératoire. Intégrer ces priorités dans les protocoles ERAS et les programmes de préadaptation pourrait améliorer la satisfaction, les expériences et les résultats chez les patients. Faire participer activement les patients à leurs soins pourrait contribuer à soulager une part de l’anxiété et de la peur associées à l’attente passive de la chirurgie.
© 2021 CMA Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Greg Nelson is secretary of the ERAS Society. He reports consulting fees from Abbott Laboratories and speaker fees from Medtronic, outside the submitted work. Olle Ljungqvist is chairman of the ERAS Society. He founded and owns stock in Encare and has received honoraria, including travel support, for advice and lecturing from Nutricia, Fresenius Kabi, Pharmacosmos and Encare, and lecturing honoraria from Medtronic and B. Braun, outside the submitted work. No other competing interests were declared.
Figures
References
-
- Gustafsson UO, Scott MJ, Hubner M, et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations: 2018. World J Surg 2019;43:659–95. - PubMed
-
- Ljungqvist O, Scott M, Fearon KC. Enhanced Recovery After Surgery: a review. JAMA Surg 2017;152:292–8. - PubMed
-
- Nelson G, Kiyang LN, Crumley ET, et al. Implementation of Enhanced Recovery After Surgery (ERAS) across a provincial healthcare system: the ERAS Alberta colorectal surgery experience. World J Surg 2016;40:1092–103. - PubMed
-
- Carli F. Physiologic considerations of Enhanced Recovery After Surgery (ERAS) programs: implications of the stress response. Can J Anaesth 2015;62:110–9. - PubMed
-
- Carli F, Gillis C, Scheede-Bergdahl C. Promoting a culture of prehabilitation for the surgical cancer patient. Acta Oncol 2017;56:128–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous