

All-cause mortality in systemic rheumatic diseases under treatment compared with the general population, 2015-2019
- PMID: 34728554
- PMCID: PMC8565571
- DOI: 10.1136/rmdopen-2021-001694
All-cause mortality in systemic rheumatic diseases under treatment compared with the general population, 2015-2019
Abstract
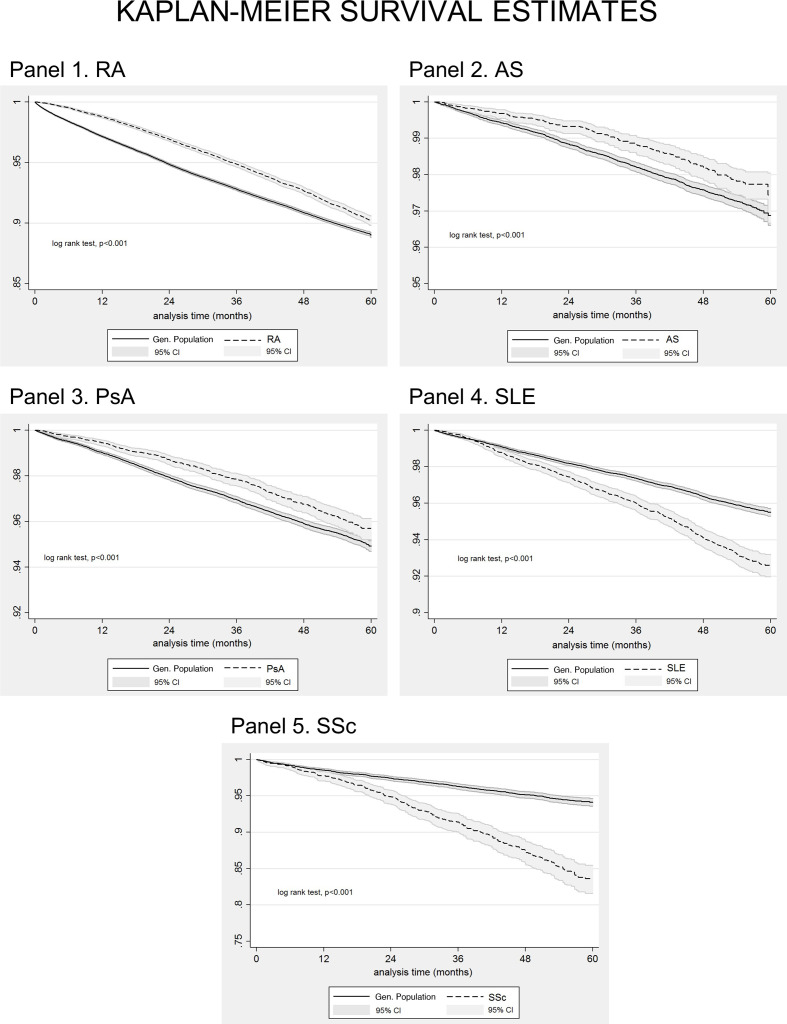
Objectives: To compare current all-cause mortality rates in rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), systemic lupus erythematosus (SLE) and systemic sclerosis (SSc) versus general population.
Methods: In this population-based, retrospective cohort study, anonymised data on 11 186 586 citizens, including all patients with RA (42 735, 79% female), AS (9707, 43% female), PsA (13 779, 55% female), SLE (10 440, 89% female) and SSc (2277, 88% female), (median age of 64/47/54/53/59 years at study entry, respectively), under prescribed treatment between 2015 and 2019, were extracted from the electronic database covering nearly 99% of the Greek population.
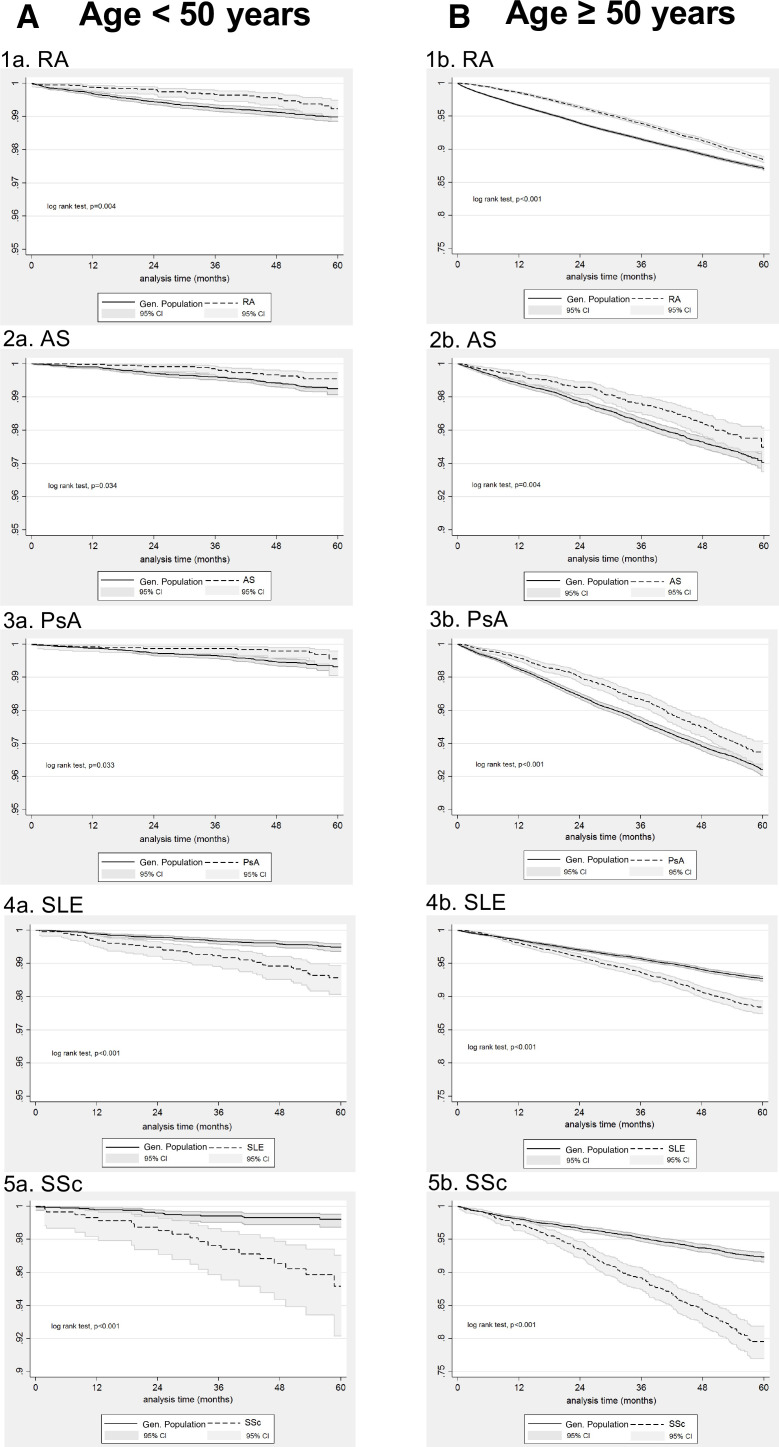
Results: After 1:5 (patients:general population) matching for gender/age, we found that survival was worse in SSc, followed by SLE and inflammatory arthritis. Compared with the general population HRs for death increased from the first 3 years to 5 years of observation possibly due to increases in disease duration: RA (from 0.63 to 1.13 (95% CI: 1.05 to 1.22), AS (from 0.62 to 1.01, (95% CI: 0.76 to 1.33)), PsA (from 0.68 to 1.06, (95% CI: 0.88 to 1.28)), SLE (from 1.52 to 1.98, (95% CI: 1.67 to 2.33)) and SSc (from 2.27 to 4.24, (95% CI: 3.19 to 5.63)). In both SLE and SSc mortality was increased in men than women and in patients younger than 50 years.
Conclusions: Survival rates over 5 years in inflammatory arthritis under treatment are currently becoming comparable (AS/PsA) or slightly higher (RA) than those of the general population. However, all-cause mortality is almost twofold and fourfold higher in SLE and SSc, respectively, being even higher for male and younger patients.
Keywords: ankylosing; arthritis; psoriatic; rheumatoid arthritis; spondylitis; systemic lupus erythematosus; systemic sclerosis.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous