

Intraoperative DNA methylation classification of brain tumors impacts neurosurgical strategy
- PMID: 34729487
- PMCID: PMC8557693
- DOI: 10.1093/noajnl/vdab149
Intraoperative DNA methylation classification of brain tumors impacts neurosurgical strategy
Abstract
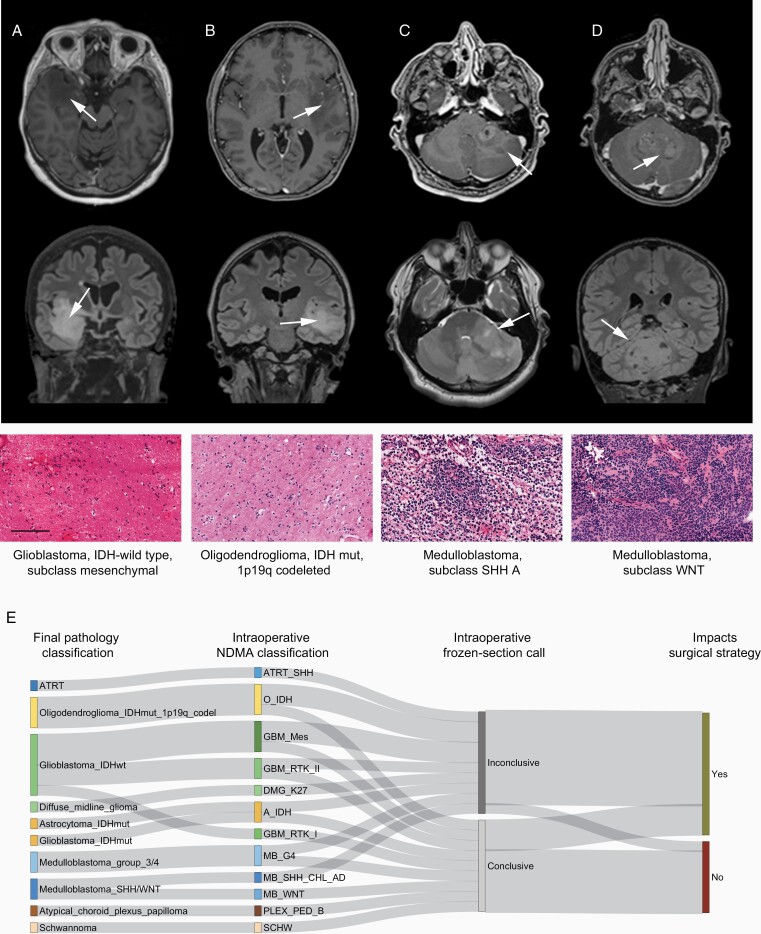
Background: Brain tumor surgery must balance the benefit of maximal resection against the risk of inflicting severe damage. The impact of increased resection is diagnosis-specific. However, the precise diagnosis is typically uncertain at surgery due to limitations of imaging and intraoperative histomorphological methods. Novel and accurate strategies for brain tumor classification are necessary to support personalized intraoperative neurosurgical treatment decisions. Here, we describe a fast and cost-efficient workflow for intraoperative classification of brain tumors based on DNA methylation profiles generated by low coverage nanopore sequencing and machine learning algorithms.
Methods: We evaluated 6 independent cohorts containing 105 patients, including 50 pediatric and 55 adult patients. Ultra-low coverage whole-genome sequencing was performed on nanopore flow cells. Data were analyzed using copy number variation and ad hoc random forest classifier for the genome-wide methylation-based classification of the tumor.
Results: Concordant classification was obtained between nanopore DNA methylation analysis and a full neuropathological evaluation in 93 of 105 (89%) cases. The analysis demonstrated correct diagnosis in 6/6 cases where frozen section evaluation was inconclusive. Results could be returned to the operating room at a median of 97 min (range 91-161 min). Precise classification of the tumor entity and subtype would have supported modification of the surgical strategy in 12 out of 20 patients evaluated intraoperatively.
Conclusion: Intraoperative nanopore sequencing combined with machine learning diagnostics was robust, sensitive, and rapid. This strategy allowed DNA methylation-based classification of the tumor to be returned to the surgeon within a timeframe that supports intraoperative decision making.
Keywords: DNA methylation; brain tumor; extent of resection; intraoperative diagnostics; nanopore.
© The Author(s) 2021. Published by Oxford University Press, the Society for Neuro-Oncology and the European Association of Neuro-Oncology.
Figures


References
-
- Duffau H, Mandonnet E. The “onco-functional balance” in surgery for diffuse low-grade glioma: integrating the extent of resection with quality of life. Acta Neurochir (Wien). 2013;155(6):951–957. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources