

ATTR Amyloidosis: Current and Emerging Management Strategies: JACC: CardioOncology State-of-the-Art Review
- PMID: 34729521
- PMCID: PMC8543085
- DOI: 10.1016/j.jaccao.2021.06.006
ATTR Amyloidosis: Current and Emerging Management Strategies: JACC: CardioOncology State-of-the-Art Review
Abstract
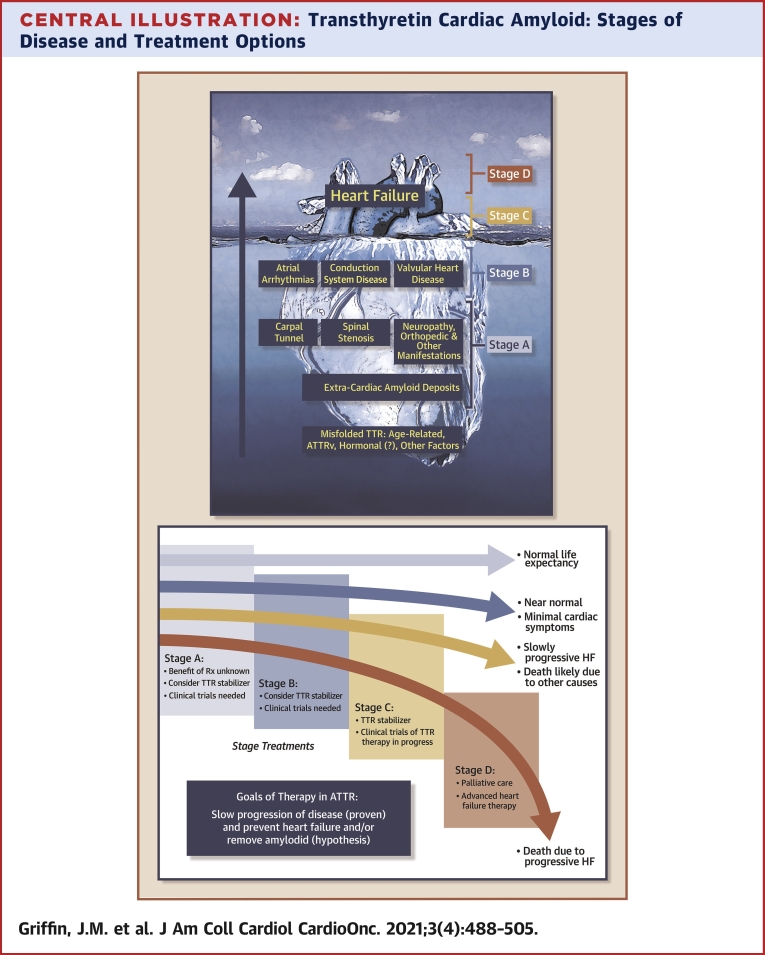
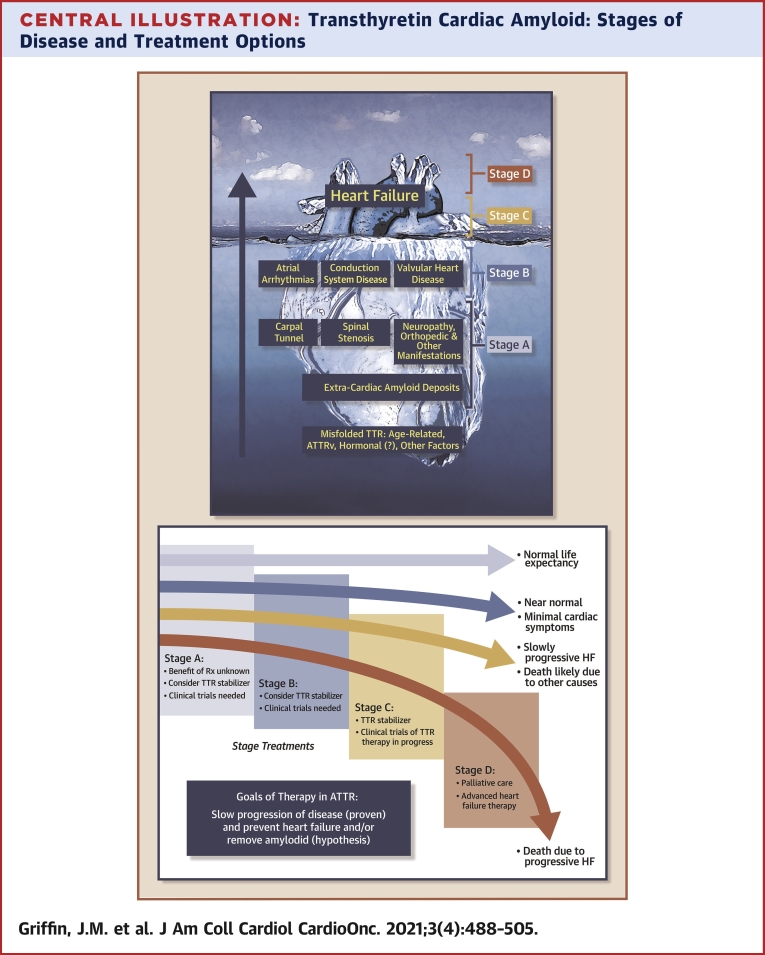
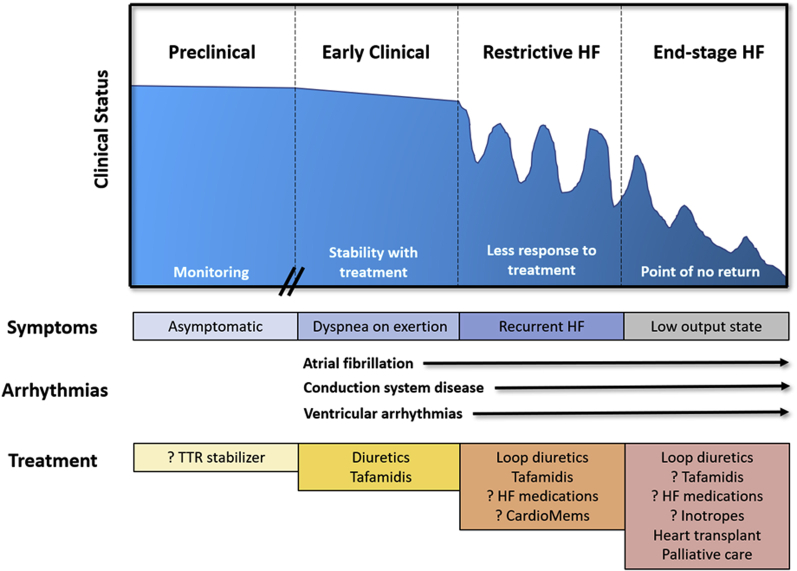
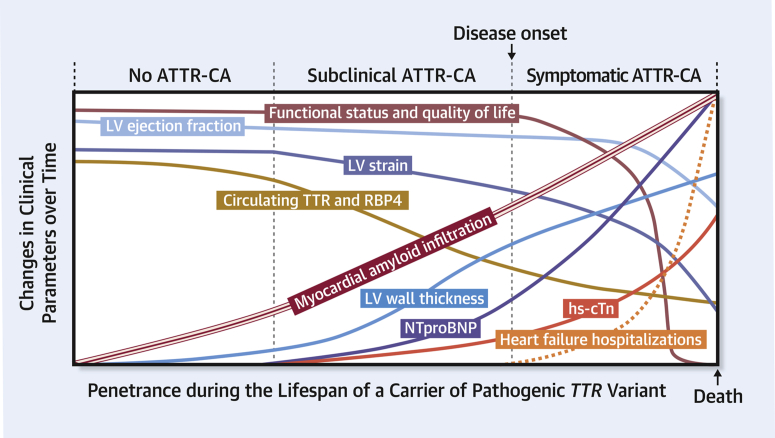
Transthyretin cardiac amyloidosis (ATTR-CA) is increasingly diagnosed owing to the emergence of noninvasive imaging and improved awareness. Clinical penetrance of pathogenic alleles is not complete and therefore there is a large cohort of asymptomatic transthyretin variant carriers. Screening strategies, monitoring, and treatment of subclinical ATTR-CA requires further study. Perhaps the most important translational triumph has been the development of effective therapies that have emerged from a biological understanding of ATTR-CA pathophysiology. These include recently proven strategies of transthyretin protein stabilization and silencing of transthyretin production. Data on neurohormonal blockade in ATTR-CA are limited, with the primary focus of medical therapy on judicious fluid management. Atrial fibrillation is common and requires anticoagulation owing to the propensity for thrombus formation. Although conduction disease and ventricular arrhythmias frequently occur, little is known regarding optimal management. Finally, aortic stenosis and ATTR-CA frequently coexist, and transcatheter valve replacement is the preferred treatment approach.
Keywords: 6MWT, 6-minute walk test; AF, atrial fibrillation; AL, light chain amyloid; AS, aortic stenosis; ASO, antisense oligonucleotide; ATTR-CA, transthyretin cardiac amyloidosis; ATTRv, variant transthyretin cardiac amyloidosis; ATTRwt, wild-type transthyretin cardiac amyloidosis; CMR, cardiac magnetic resonance; DCCV, direct current cardioversion; HF, heart failure; LVEF, left ventricular ejection fraction; NT-proBNP, N-terminal pro–B-type natriuretic peptide; SAP, serum amyloid P component; TAVR, transcatheter aortic valve replacement; amyloidosis; cardiomyopathy; heart failure; siRNA, small interfering RNA.
© 2021 The Authors.
Conflict of interest statement
Dr Grodin has received personal fees from Pfizer, Alnylam, and Eidos; and has received grant support from the Texas Health Resources Clinical Scholarship and Eidos. Dr Maurer has received grant support from the National Institutes of Health (R01HL139671-01, R21AG058348, and K24AG036778); has received consulting income from Pfizer, GlaxoSmithKline, Intellia, EIdos, Prothena, Akcea, and Alnylam; and his institution has received clinical trial funding from Pfizer, Prothena, Eidos, and Alnylam. Dr Grogan has received research (clinical trial) grant support from Alnylam, Eidos, Pfizer, and Prothena; and has received consulting fees and honoraria paid to Mayo Clinic (no personal compensation) from Akcea, Alnylam, Eidos, Pfizer, and Prothena. Dr Cheng has received grant support from the National Institutes of Health (R21HL152149); and his institution has received clinical trial funding from Eidos and Ionis. Dr Rosenthal has received research (clinical trial) grant support from Akcea; and has received consulting fees from Pfizer. Dr Griffin has reported that he has no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Witteles R.M., Bokhari S., Damy T. Screening for transthyretin amyloid cardiomyopathy in everyday practice. J Am Coll Cardiol HF. 2019;7:709–716. - PubMed
-
- Gillmore J.D., Maurer M.S., Falk R.H. Nonbiopsy diagnosis of cardiac transthyretin amyloidosis. Circulation. 2016;133:2404–2412. - PubMed
-
- Gonzalez-Lopez E., Gallego-Delgado M., Guzzo-Merello G. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection fraction. Eur Heart J. 2015;36:2585–2594. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
