

Physiologically based pharmacokinetic modeling for dose optimization of quinine-phenobarbital coadministration in patients with cerebral malaria
- PMID: 34730282
- PMCID: PMC8752110
- DOI: 10.1002/psp4.12737
Physiologically based pharmacokinetic modeling for dose optimization of quinine-phenobarbital coadministration in patients with cerebral malaria
Abstract
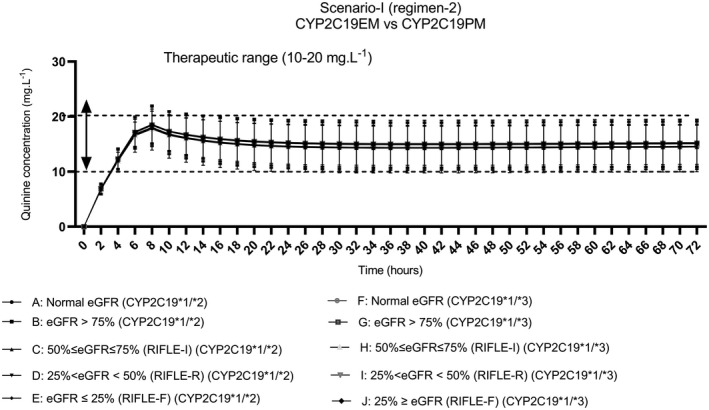
Patients with cerebral malaria with polymorphic Cytochrome P450 2C19 (CYP2C19) genotypes who receive concurrent treatment with quinine are at risk of inadequate or toxic therapeutic drug concentrations due to metabolic drug interactions. The study aimed to predict the potential dose regimens of quinine when coadministered with phenobarbital in adult patients with cerebral malaria and complications (e.g., lactic acidosis and acute renal failure) and concurrent with seizures and acute renal failure who carry wild-type and polymorphic CYP2C19. The whole-body physiologically based pharmacokinetic (PBPK) models for quinine, phenobarbital, and quinine-phenobarbital coadministration were constructed based on the previously published information using Simbiology®. Four published articles were used for model validation. A total of 100 virtual patients were simulated based on the 14-day and 3-day courses of treatment. using the drug-drug interaction approach. The predicted results were within 15% of the observed values. Standard phenobarbital dose, when administered with quinine, is suitable for all groups with single or continuous seizures regardless of CYP2C19 genotype, renal failure, and lactic acidosis. Dose adjustment based on area under the curve ratio provided inappropriate quinine concentrations. The recommended dose of quinine when coadministered with phenobarbital based on the PBPK model for all groups is a loading dose of 2000 mg intravenous (i.v.) infusion rate 250 mg/h followed by 1200 mg i.v. rate 150 mg/h. The developed PBPK models are credible for further simulations. Because the predicted quinine doses in all groups were similar regardless of the CYP2C19 genotype, genotyping may not be required.
© 2021 The Authors. CPT: Pharmacometrics & Systems Pharmacology published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
The authors declared no conflict of interest.
Figures




References
-
- Durrani AB, Durrani IU, Abbas N, Jabeen M. Epidemiology of cerebral malaria and its mortality. J Pak Med Assoc. 1997;47(8):213‐215. - PubMed
-
- Idro R, Jenkins NE, Newton CR. Pathogenesis, clinical features, and neurological outcome of cerebral malaria. Lancet Neurol. 2005;4(12):827‐840. - PubMed
-
- Chisholm D, Who C. Cost‐effectiveness of first‐line antiepileptic drug treatments in the developing world: a population‐level analysis. Epilepsia. 2005;46(5):751‐759. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
