

Association Between Melanoma Detected During Routine Skin Checks and Mortality
- PMID: 34730781
- PMCID: PMC8567188
- DOI: 10.1001/jamadermatol.2021.3884
Association Between Melanoma Detected During Routine Skin Checks and Mortality
Abstract
Importance: Early melanoma diagnosis is associated with better health outcomes, but there is insufficient evidence that screening, such as having routine skin checks, reduces mortality.
Objective: To assess melanoma-specific and all-cause mortality associated with melanomas detected through routine skin checks, incidentally or patient detected. A secondary aim was to examine patient, sociodemographic, and clinicopathologic factors associated with different modes of melanoma detection.
Design, setting, and participants: This prospective, population-based, cohort study included patients in New South Wales, Australia, who were diagnosed with melanoma over 1 year from October 23, 2006, to October 22, 2007, in the Melanoma Patterns of Care Study and followed up until 2018 (mean [SD] length of follow-up, 11.9 [0.3] years) by using linked mortality and cancer registry data. All patients who had invasive melanomas recorded at the cancer registry were eligible for the study, but the number of in situ melanomas was capped. The treating doctors recorded details of melanoma detection and patient and clinical characteristics in a baseline questionnaire. Histopathologic variables were obtained from pathology reports. Of 3932 recorded melanomas, data were available and analyzed for 2452 (62%; 1 per patient) with primary in situ (n = 291) or invasive (n = 2161) cutaneous melanoma. Data were analyzed from March 2020 to January 2021.
Main outcomes and measures: Melanoma-specific mortality and all-cause mortality.
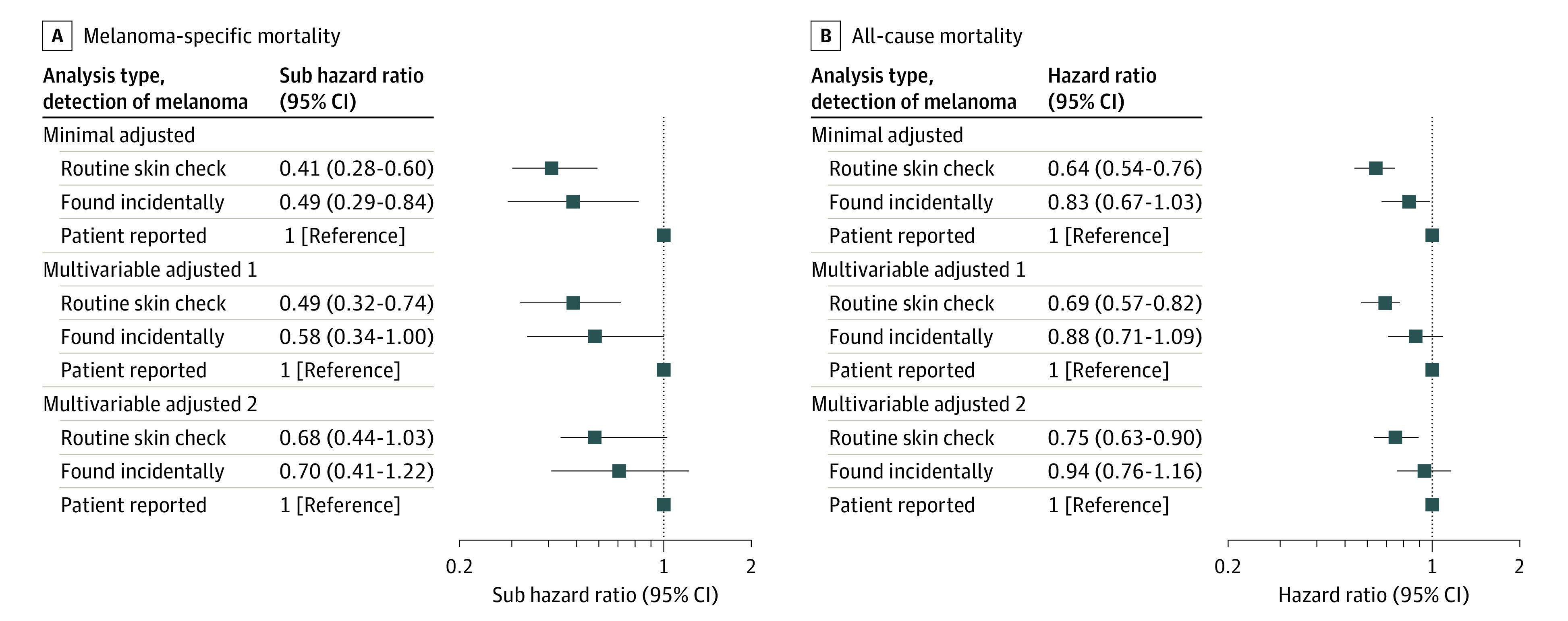
Results: A total of 2452 patients were included in the analyses. The median age at diagnosis was 65 years (range, 16-98 years), and 1502 patients (61%) were men. A total of 858 patients (35%) had their melanoma detected during a routine skin check, 1148 (47%) self-detected their melanoma, 293 (12%) had their melanoma discovered incidentally when checking another skin lesion, and 153 (6%) reported "other" presentation. Routine skin-check detection of invasive melanomas was associated with 59% lower melanoma-specific mortality (subhazard ratio, 0.41; 95% CI, 0.28-0.60; P < .001) and 36% lower all-cause mortality (hazard ratio, 0.64; 95% CI, 0.54-0.76; P < .001), adjusted for age and sex, compared with patient-detected melanomas. After adjusting for prognostic factors including ulceration and mitotic rate, the associations were 0.68 (95% CI, 0.44-1.03; P = .13), and 0.75 (95% CI, 0.63-0.90; P = .006), respectively. Factors associated with higher odds of routine skin-check melanoma detection included being male (female vs male, odds ratio [OR], 0.73; 95% CI, 0.60-0.89; P = .003), having previous melanoma (vs none, OR, 2.36; 95% CI, 1.77-3.15; P < .001), having many moles (vs not, OR, 1.39; 95% CI, 1.10-1.77; P = .02), being 50 years or older (eg, 50-59 years vs <40 years, OR, 2.89; 95% CI, 1.92-4.34; P < .001), and living in nonremote areas (eg, remote or very remote vs major cities, OR, 0.23; 95% CI, 0.05-1.04; P = .003).
Conclusions and relevance: In this cohort study, melanomas diagnosed through routine skin checks were associated with significantly lower all-cause mortality, but not melanoma-specific mortality, after adjustment for patient, sociodemographic, and clinicopathologic factors.
Conflict of interest statement
Figures
Comment in
-
Melanoma Screening-Time for a Reset?JAMA Dermatol. 2021 Dec 1;157(12):1409-1411. doi: 10.1001/jamadermatol.2021.3883. JAMA Dermatol. 2021. PMID: 34730779 No abstract available.
References
-
- Gershenwald JE, Scolyer RA, Hess KR, et al. ; for members of the American Joint Committee on Cancer Melanoma Expert Panel and the International Melanoma Database and Discovery Platform . Melanoma staging: evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(6):472-492. doi: 10.3322/caac.21409 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
