

Sleep, Pain, and Cognition: Modifiable Targets for Optimal Perioperative Brain Health
- PMID: 34731233
- PMCID: PMC8578455
- DOI: 10.1097/ALN.0000000000004046
Sleep, Pain, and Cognition: Modifiable Targets for Optimal Perioperative Brain Health
Abstract
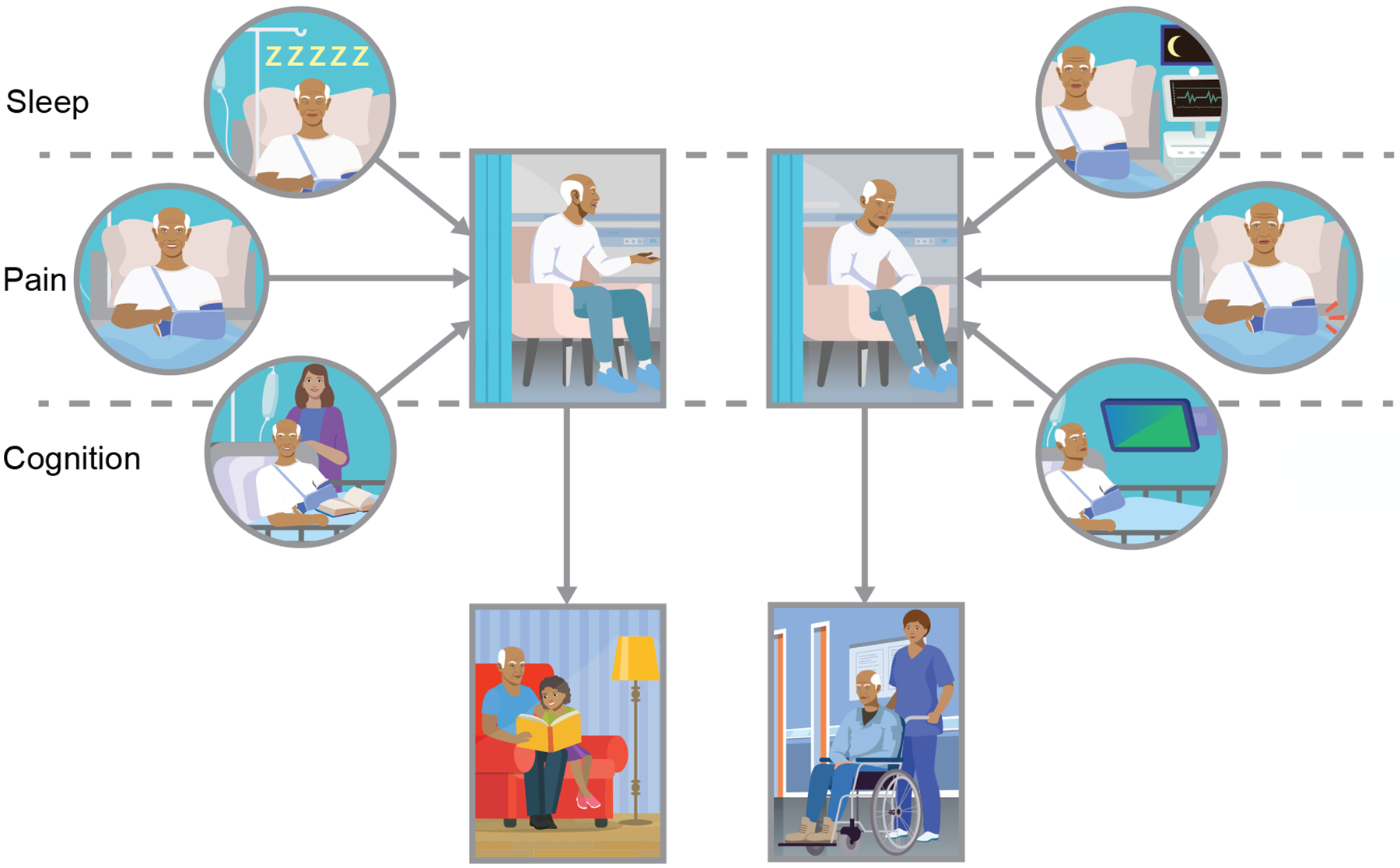
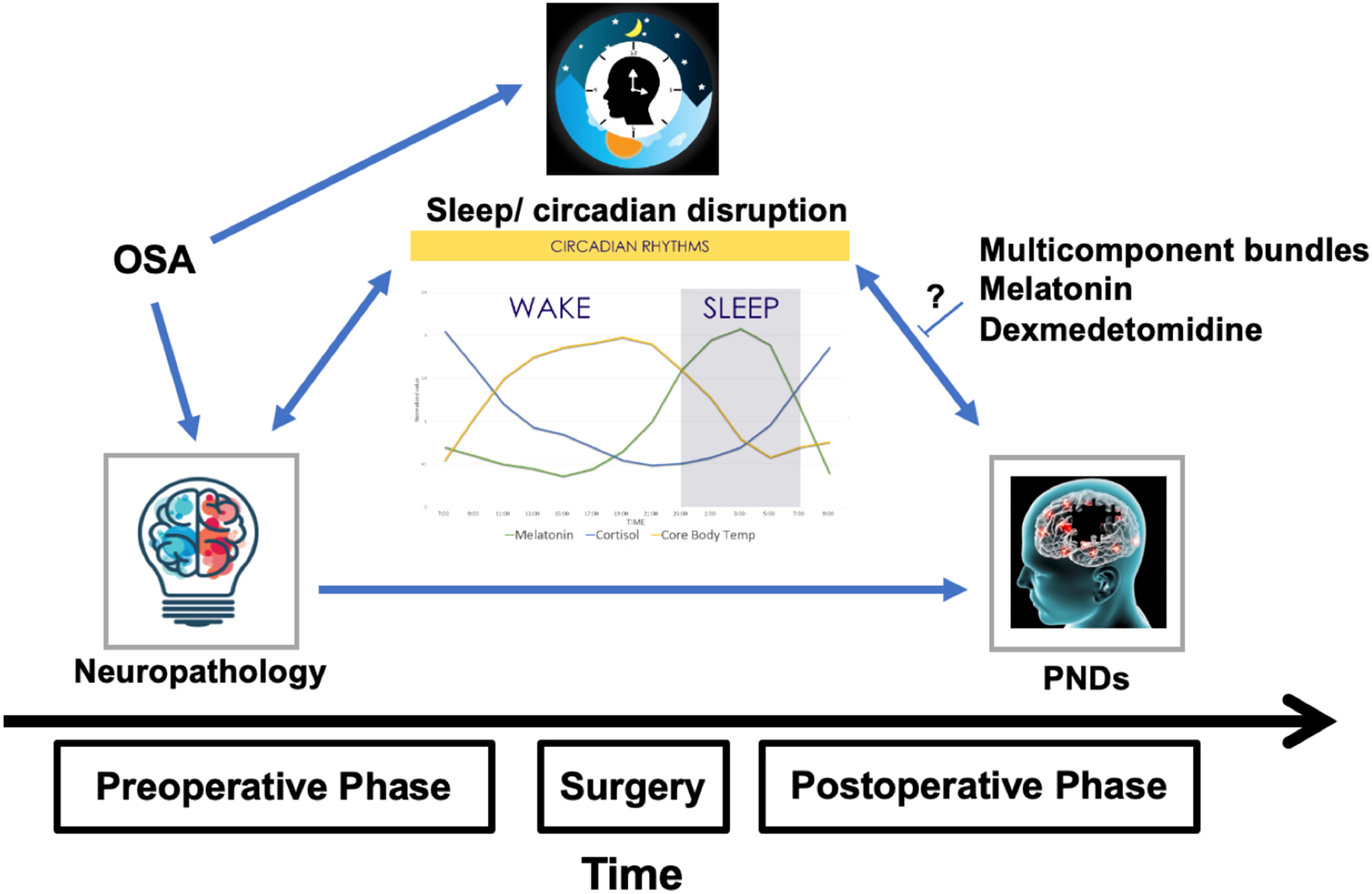
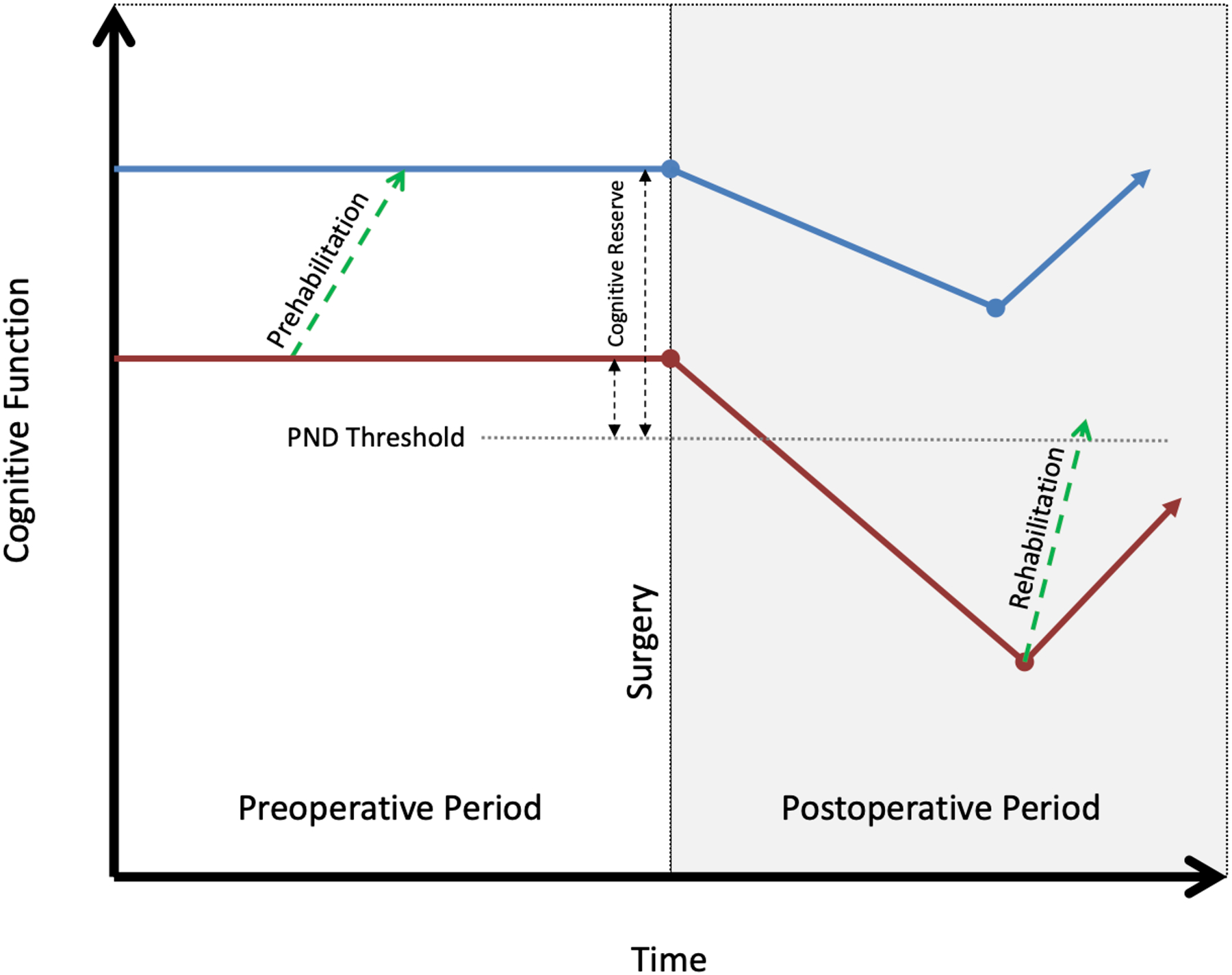
The prevention of perioperative neurocognitive disorders is a priority for patients, families, clinicians, and researchers. Given the multiple risk factors present throughout the perioperative period, a multicomponent preventative approach may be most effective. The objectives of this narrative review are to highlight the importance of sleep, pain, and cognition on the risk of perioperative neurocognitive disorders and to discuss the evidence behind interventions targeting these modifiable risk factors. Sleep disruption is associated with postoperative delirium, but the benefit of sleep-related interventions is uncertain. Pain is a risk factor for postoperative delirium, but its impact on other postoperative neurocognitive disorders is unknown. Multimodal analgesia and opioid avoidance are emerging as best practices, but data supporting their efficacy to prevent delirium are limited. Poor preoperative cognitive function is a strong predictor of postoperative neurocognitive disorder, and work is ongoing to determine whether it can be modified to prevent perioperative neurocognitive disorders.
Copyright © 2021, the American Society of Anesthesiologists. All Rights Reserved.
Conflict of interest statement
Conflicts of Interest:
Dr. O’Gara receives consulting income from Sedana Medical for work unrelated to this review. He and the other authors declare no competing interests.
Figures

References
-
- Evered L, Silbert B, Knopman DS, Scott DA, DeKosky ST, Rasmussen LS, Oh ES, Crosby G, Berger M, Eckenhoff RG: Recommendations for the Nomenclature of Cognitive Change Associated with Anaesthesia and Surgery-2018. Anesthesiology 2018; 129: 872–879 - PubMed
-
- Mahanna-Gabrielli E, Schenning KJ, Eriksson LI, Browndyke JN, Wright CB, Evered L, Scott DA, Wang NY, Brown CH, Oh E, Purdon P, Inouye S, Berger M, Whittington RA, Deiner S: State of the clinical science of perioperative brain health: report from the American Society of Anesthesiologists Brain Health Initiative Summit 2018. British Journal of Anaesthesia 2019; 123: 464–478 - PMC - PubMed
-
- Sprung J, Roberts RO, Weingarten TN, Nunes Cavalcante A, Knopman DS, Petersen RC, Hanson AC, Schroeder DR, Warner DO: Postoperative delirium in elderly patients is associated with subsequent cognitive impairment. Br J Anaesth 2017; 119: 316–323 - PubMed
-
- Evered LA, Silbert BS: Postoperative Cognitive Dysfunction and Noncardiac Surgery. Anesth Analg 2018; 127: 496–505 - PubMed
