Characterisation of trocar associated gas leaks during laparoscopic surgery
- PMID: 34731302
- PMCID: PMC8565170
- DOI: 10.1007/s00464-021-08807-1
Characterisation of trocar associated gas leaks during laparoscopic surgery
Erratum in
-
Correction to: Characterisation of trocar associated gas leaks during laparoscopic surgery.Surg Endosc. 2022 Jun;36(6):4552. doi: 10.1007/s00464-021-08897-x. Surg Endosc. 2022. PMID: 34812924 Free PMC article. No abstract available.
Abstract
Background: During laparoscopy, the abdominal cavity is insufflated with carbon dioxide (CO2) that could become contaminated with viruses and surgical smoke. Medical staff is potentially exposed when this gas leaks into the operating room through the instruments and past trocar valves. No detailed studies currently exist that have quantified these leakage pathways. Therefore, the goal of this study was to quantify the gas leakages through trocars and instruments, during minimally invasive procedures.
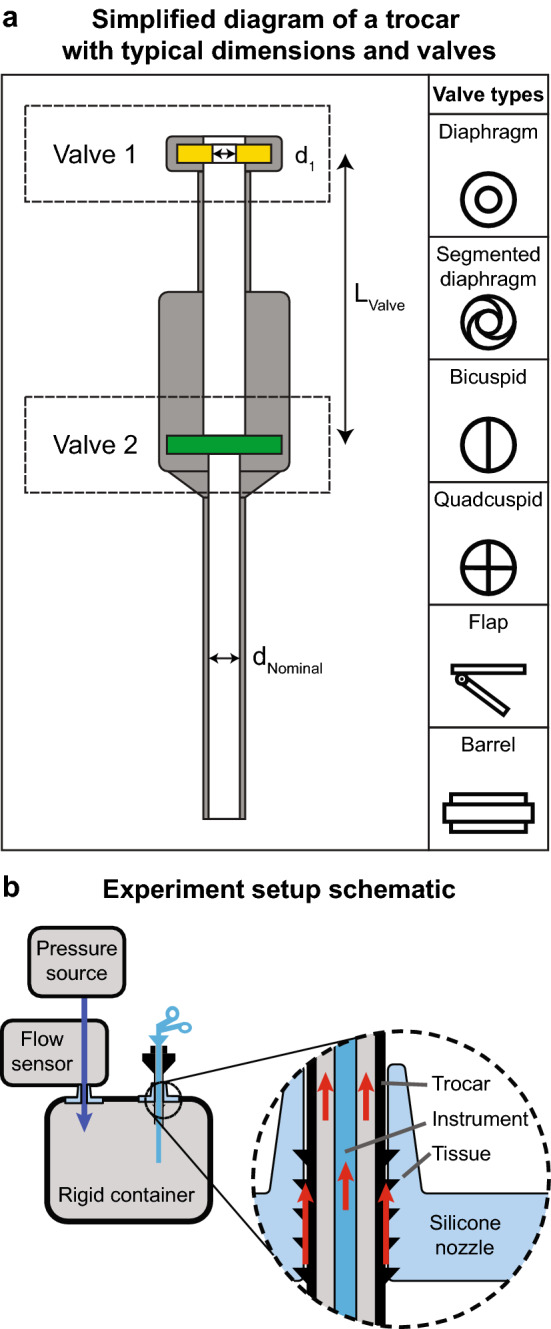
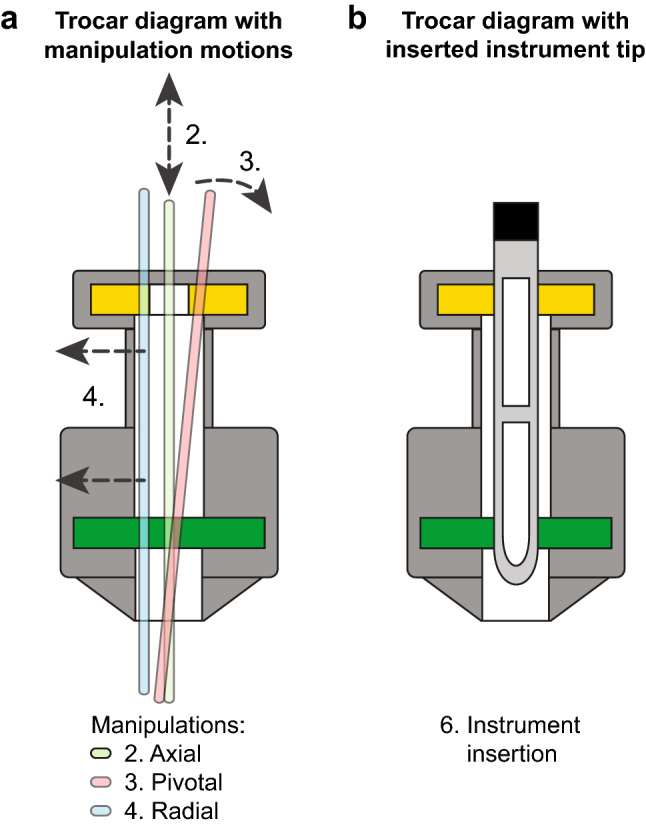
Methods: A model of the surgical environment was created, consisting of a rigid container with an interface for airtight clamping of laparoscopic equipment such as trocars and surgical instruments. The model was insufflated to 15 mm Hg using a pressure generator and a pneumotachograph measured the equipment gas leak. A protocol of several use cases was designed to simulate the motions and forces the surgeon exerts on the trocar during surgery.
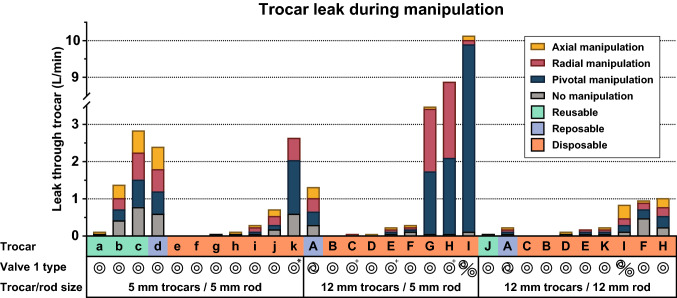
Results: Twenty-three individual trocars and twenty-six laparoscopic instruments were measured for leakage under the different conditions of the protocol. Trocar leakages varied between 0 L/min and more than 30 L/min, the instruments revealed a range of leakages between 0 L/min and 5.5 L/min. The results showed that leakage performance varied widely between trocars and instruments and that the performance and location of the valves influenced trocar leakage.
Conclusions: We propose trocar redesigns to overcome specific causes of gas leaks. Moreover, an international testing standard for CO2 leakage for all new trocars and instruments is needed so surgical teams can avoid this potential health hazard when selecting new equipment.
Keywords: Carbon dioxide; Gas leak; Laparoscopic equipment; Surgical safety; Surgical smoke.
© 2021. The Author(s).
Conflict of interest statement
Mr Daniel Robertson, Mr Frank Sterke, Mr Willem van Weteringen, Dr Alberto Arezzo, Dr Yoav Mintz, Dr Felix Nickel and Dr Tim Horeman have no conflicts of interest or financial ties to disclose.
Figures