

Hyperkalemia Risk with Finerenone: Results from the FIDELIO-DKD Trial
- PMID: 34732509
- PMCID: PMC8763180
- DOI: 10.1681/ASN.2021070942
Hyperkalemia Risk with Finerenone: Results from the FIDELIO-DKD Trial
Abstract
Background: Finerenone reduced risk of cardiorenal outcomes in patients with CKD and type 2 diabetes in the FIDELIO-DKD trial. We report incidences and risk factors for hyperkalemia with finerenone and placebo in FIDELIO-DKD.
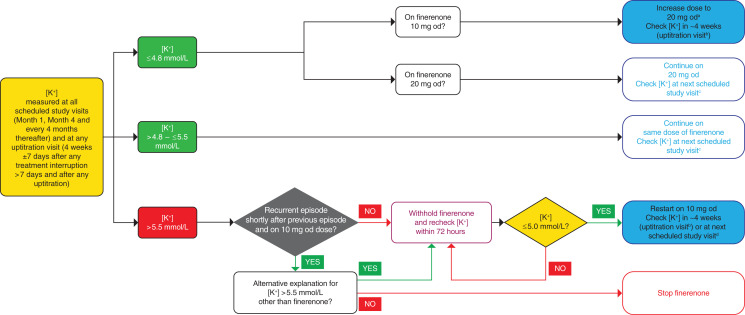
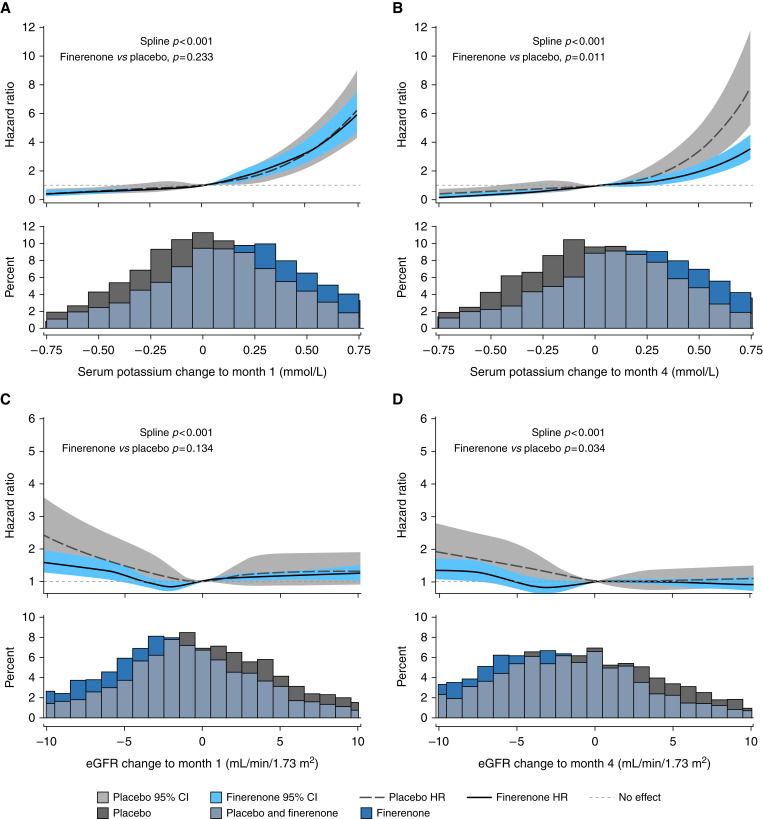
Methods: This post hoc safety analysis defined hyperkalemia as ≥mild or ≥moderate based on serum potassium concentrations of >5.5 or >6.0 mmol/L, respectively, assessed at all regular visits. Cumulative incidences of hyperkalemia were based on the Aalen-Johansen estimator using death as competing risk. A multivariate Cox proportional hazards model identified significant independent predictors of hyperkalemia. Restricted cubic splines assessed relationships between short-term post-baseline changes in serum potassium or eGFR and subsequent hyperkalemia risk. During the study, serum potassium levels guided drug dosing. Patients in either group who experienced ≥mild hyperkalemia had the study drug withheld until serum potassium was ≤5.0 mmol/L; then the drug was restarted at the 10 mg daily dose. Placebo-treated patients underwent sham treatment interruption and downtitration.
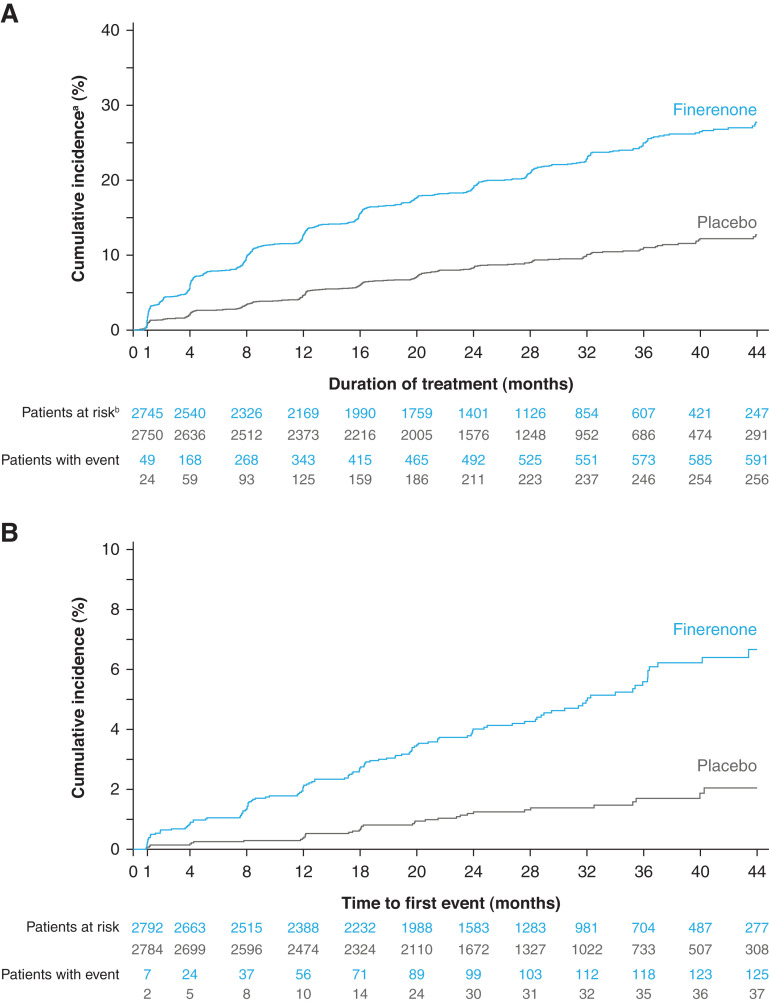
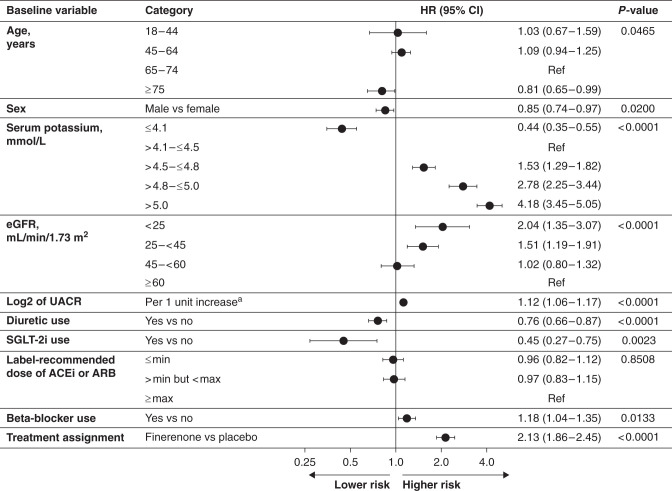
Results: Over 2.6 years' median follow-up, 597 of 2785 (21.4%) and 256 of 2775 (9.2%) patients treated with finerenone and placebo, respectively, experienced treatment-emergent ≥mild hyperkalemia; 126 of 2802 (4.5%) and 38 of 2796 (1.4%) patients, respectively, experienced moderate hyperkalemia. Independent risk factors for ≥mild hyperkalemia were higher serum potassium, lower eGFR, increased urine albumin-creatinine ratio, younger age, female sex, β-blocker use, and finerenone assignment. Diuretic or sodium-glucose cotransporter-2 inhibitor use reduced risk. In both groups, short-term increases in serum potassium and decreases in eGFR were associated with subsequent hyperkalemia. At month 4, the magnitude of increased hyperkalemia risk for any change from baseline was smaller with finerenone than with placebo.
Conclusions: Finerenone was independently associated with hyperkalemia. However, routine potassium monitoring and hyperkalemia management strategies employed in FIDELIO-DKD minimized the impact of hyperkalemia, providing a basis for clinical use of finerenone.
Keywords: chronic kidney disease; diabetic nephropathy; hyperkalemia; mineralocorticoid receptor antagonist; randomized controlled trials.
Copyright © 2022 by the American Society of Nephrology.
Figures
References
-
- Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, et al. ; RENAAL Study Investigators : Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 345: 861–869, 2001 - PubMed
-
- Lewis EJ, Hunsicker LG, Clarke WR, Berl T, Pohl MA, Lewis JB, et al. ; Collaborative Study Group : Renoprotective effect of the angiotensin-receptor antagonist irbesartan in patients with nephropathy due to type 2 diabetes. N Engl J Med 345: 851–860, 2001 - PubMed
-
- Kidney Disease: Improving Global Outcomes: KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Available at: https://kdigo.org/wp-content/uploads/2017/02/KDIGO_2012_CKD_GL.pdf. Accessed December 9, 2021
-
- Parving HH, Brenner BM, McMurray JJ, de Zeeuw D, Haffner SM, Solomon SD, et al. ; ALTITUDE Investigators : Cardiorenal end points in a trial of aliskiren for type 2 diabetes. N Engl J Med 367: 2204–2213, 2012 - PubMed
-
- Fried LF, Emanuele N, Zhang JH, Brophy M, Conner TA, Duckworth W, et al. ; VA NEPHRON-D Investigators : Combined angiotensin inhibition for the treatment of diabetic nephropathy. N Engl J Med 369: 1892–1903, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
