

Interferon Genes Are Influenced by 17β-Estradiol in SLE
- PMID: 34733276
- PMCID: PMC8558410
- DOI: 10.3389/fimmu.2021.725325
Interferon Genes Are Influenced by 17β-Estradiol in SLE
Abstract
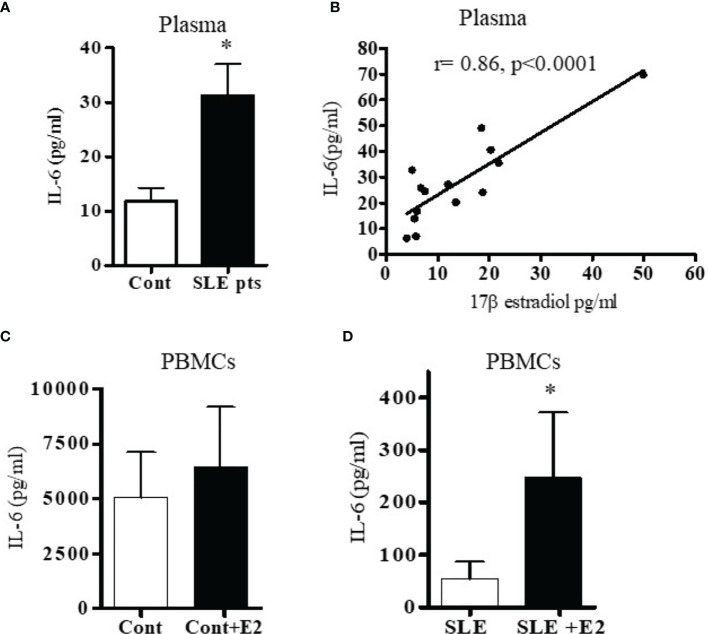
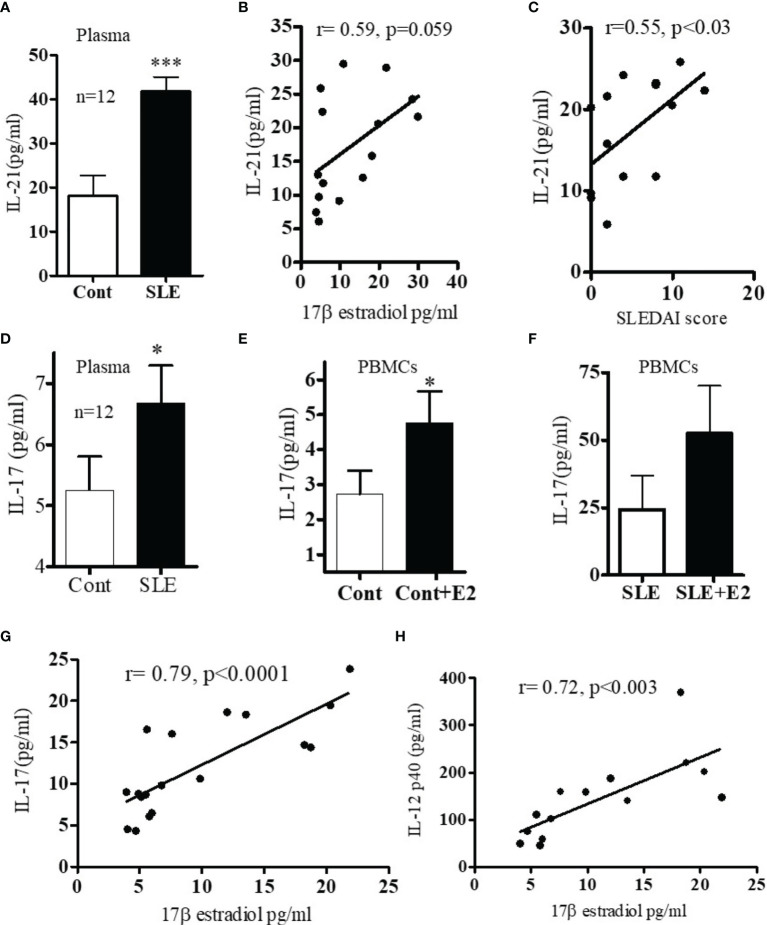
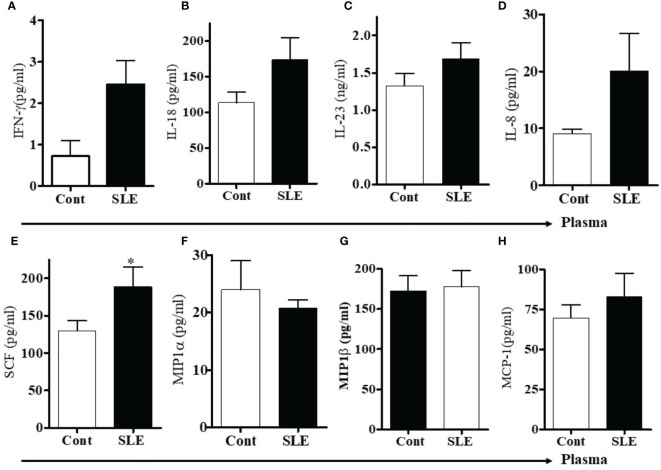
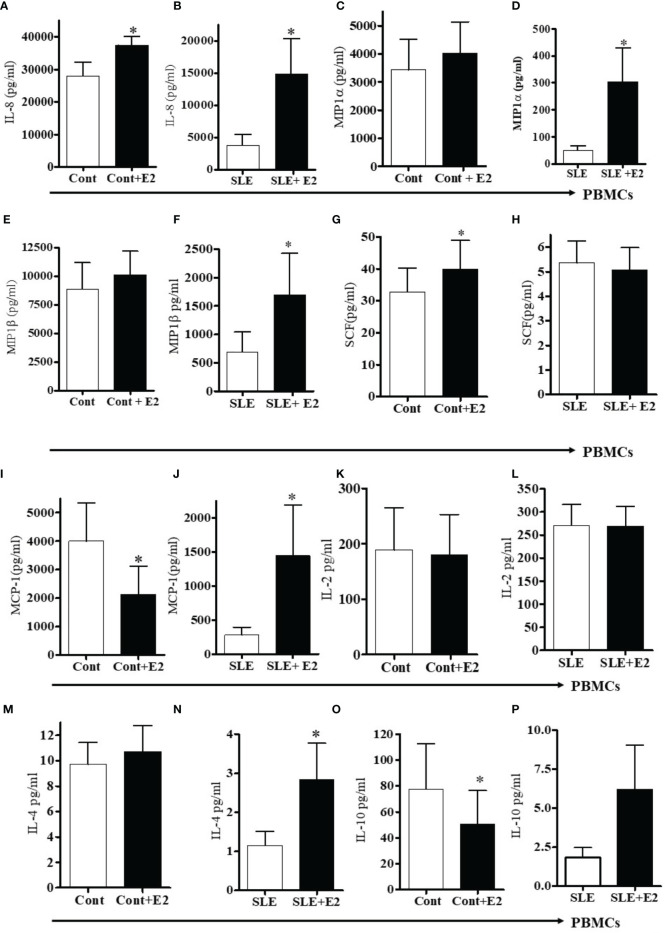
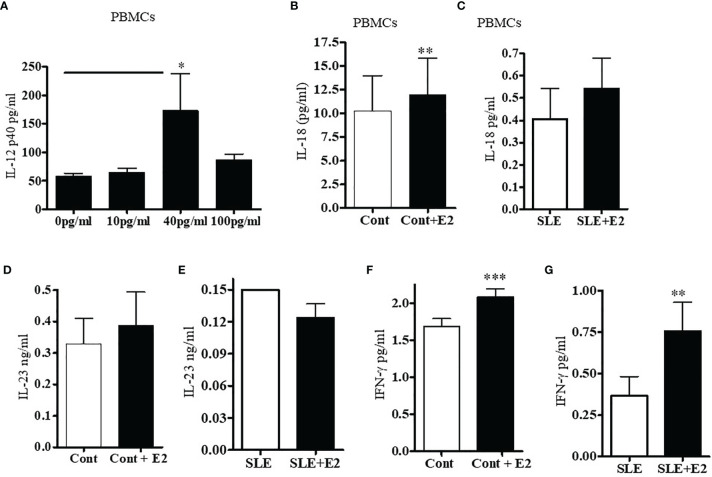
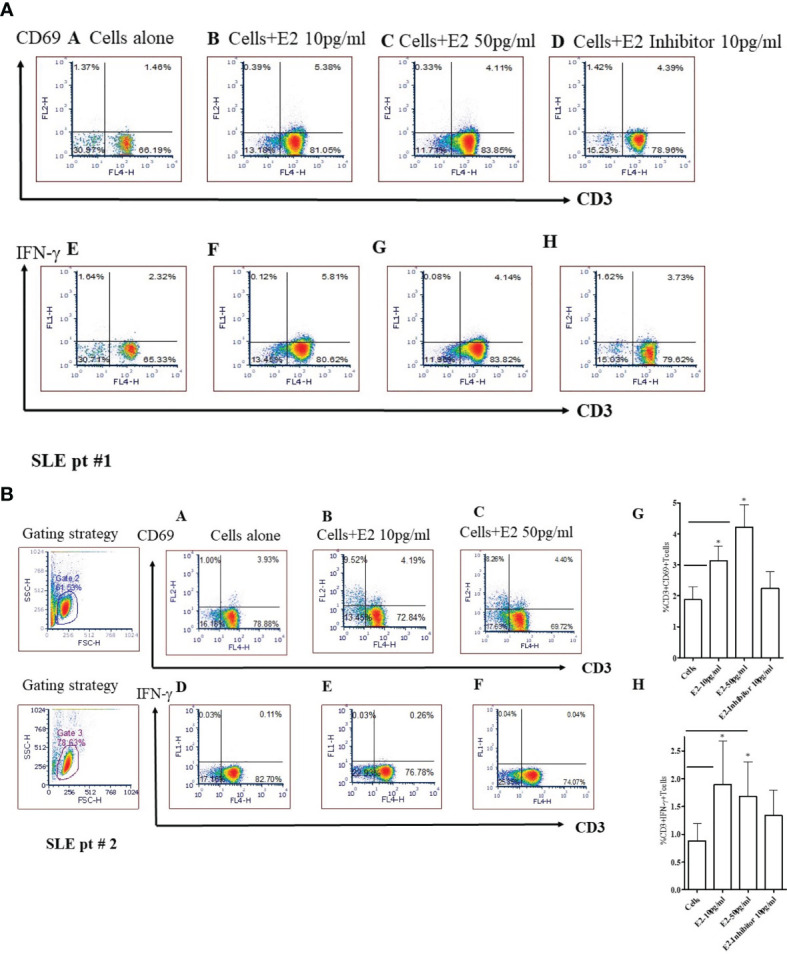
Recent evidence suggests the existence of a nexus between inflammatory pathways and the female sex hormone 17β-estradiol, resulting in increased interferon-stimulated genes (ISGs), autoantibodies, and dysregulation of immune cells in SLE. However, the molecular mechanisms and the effect of estradiol on candidate target genes and their pathways remains poorly understood. Our previous work suggests that female SLE patients have increased estradiol levels compared to healthy controls. In the present study, we explored the effects of 17β-estradiol treatment on expression of IFN (interferons)-stimulated genes and pro-inflammatory cytokines/chemokines. We found significantly increased (5-10-fold) expression of IFN-regulated genes in healthy females. Furthermore, we found significantly increased plasma levels of IL-6, IL-12, IL-17, IL-18, stem cell factor (SCF), and IL-21/IL-23 in SLE patients compared to healthy controls, and those levels positively correlated with the plasma levels of 17β-estradiol. In addition, levels of IL-21 positively correlated with the SLE disease activity index (SLEDAI) score of SLE patients. In vitro treatment of PBMCs from either SLE patients or healthy controls with 17β-estradiol at physiological concentration (~50 pg/ml) also significantly increased secretion of many pro-inflammatory cytokines and chemokines (IL-6, IL-12, IL-17, IL-8, IFN-γ; MIP1α, and MIP1β) in both groups. Further our data revealed that 17β-estradiol significantly increased the percentage of CD3+CD69+ and CD3+IFNγ+ T cells; whereas, simultaneous addition of 17β-estradiol and an ERα inhibitor prevented this effect. Collectively, our findings indicate that 17β-estradiol participates in the induction of pro-inflammatory cytokines and chemokines and further influences interferon genes and pathways.
Keywords: T cells; cytokines/chemokines; estradiol; interferon genes; systemic lupus erythematosus.
Copyright © 2021 Singh, Hahn and Bischoff.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous