

Editorial
doi: 10.1177/20406207211053120.
eCollection 2021.
Integration of cell therapies and bispecific antibodies into the treatment pathway of relapsed diffuse large B-cell lymphoma
Affiliations
- PMID: 34733463
- PMCID: PMC8558790
- DOI: 10.1177/20406207211053120
Item in Clipboard
Editorial
Integration of cell therapies and bispecific antibodies into the treatment pathway of relapsed diffuse large B-cell lymphoma
Ther Adv Hematol.
.
No abstract available
Conflict of interest statement
Conflict of interest statement: A.R. received conference fees from Gilead. G.C. received honoraria from Roche, Takeda, Gilead Sciences, Pfizer, Novartis, Daiichi Sankyo, Incyte, Celleron Therapeutics, MSD Oncology, BeiGene, and ADC Therapeutics; played consulting or advisory role in Roche, Takeda, Incyte, Pfizer, MSD, Celgene, Beigene, Daiichi Sankyo, Celleron Therapeutics, and ADC Therapeutics; as speakers’ bureau in Roche, Takeda, Novartis, and Gilead Sciences; received research funding from MSD Oncology, Celgene, Celleron Therapeutics, Bristol-Myers Squibb, and Amgen; received travel and accommodations expenses from Roche and Takeda. GS: No conflicts of interest
Figures
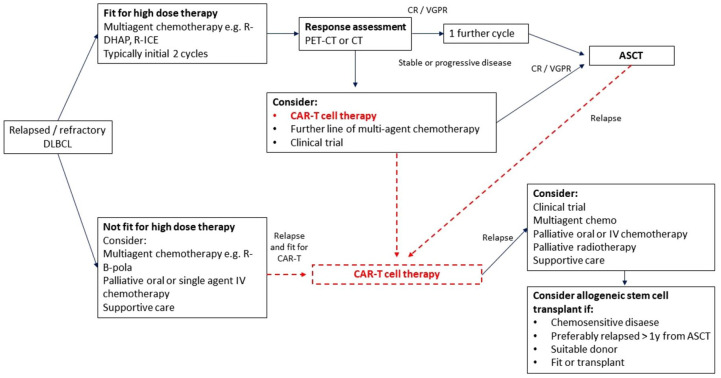
Pathway for relapsed/refractory DLBCL. ASCT, autologous stem cell transplantation; CAR-T, chimeric antigen receptors-T cells; CR, complete response; CT, cell transplantation; DLBCL, diffuse large B-cell lymphoma; PET, positron emmission tomography; R-B-pola, rituximab, Bendamustine, polatuzumab vedotin; R-DHAP, rituximab, dexamethasone, cytarabine, cisplatin; R-ICE, rituximab, ifosfamide, carboplatin, etoposide; VGPR, very good partial response.

Step 1: Collecting CD3+ T-cell apheresis from the patient is the first step towards making the CAR T product. A minimum of 0.6 × 10*9 and an ideal of 2 × 10*9 cells is usually required. Although the number of cells required is not very high, these patients are often pretreated with steroid, monoclonal antibodies and cytotoxic medication that renders them lymphopenic and this can make harvesting adequate numbers of cells challenging. Despite this, in a cohort of 71 patients, the minimum cell dose was achieved in 97% and the ideal target in 77% of the patients. Step 2: The collected product is washed and the collected T-cells are activated and expanded by various techniques, a process that enables them to obtain a memory phenotype and become less resistance to transduction A lentivirus or retrovirus vector is used to insert the genetic material into the T-cells. Step 3: The genetic material is incorporated into the T-cells’ DNA transforming them into a chimeric receptor T-cells. This genetic material expresses a single chain fragment anti CD19 which is connected to a co-stimulatory transmembrane molecule (either CD28 or 4-1BB) and a CD3-ζ chain which is the cytoplasmic signalling domain that will activate the T-cell. Step 4: The cells are re-infused to the patient. Step 5: Within a few days the CAR-T identify their target, become activated and expand. This can be monitored by flow cytometry as CAR-Ts carry a specific signature, while other markers on their surface determine their status (fatigue, activity, etc). The time of activation, the level of expansion and the persistence in the blood may be determined by the co-stimulatory molecule of each product. Step 5: The CAR-T cells induce a strong immunological response. This immunological response is driven by a cytokine release of TNFa, Interleukin-6, interferon-γ, while it also attracts other cells, mainly macrophages which contribute to the immune response. The tenacity of this phenomenon can determine the severity of cytokine release syndrome which is one of the main CAR-T-related toxicities. CAR-T, chimeric antigen receptors-T cells; DNA, deoxyribonucleic acid; VH, variable heavy chain; VL variable light chain.

Bispecific antibodies comparison to Bispecific T-cell Engager. BiTEs target a tumour-specific antigen and CD3 which is present in T-cells ‘bringing them’ together and facilitating an immune response by the T-cell towards the tumour. BSAs work in a similar manner, but they also retain the Fc receptor which enables them to induce a broader immune response by other immune effector cells as well. Their larger size makes them less prone to renal excretion avoiding the need for a continuous infusion that BiTEs require. BiTE, bi-specific T-cell engager; BSA, bispecific antibodies.
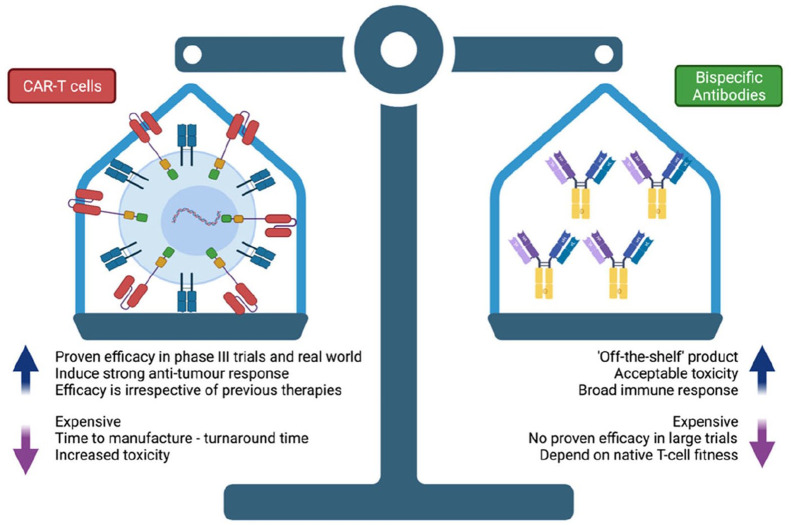
Benefits and limitations of CAR-T cells and bispecific antibodies. CAR-T, chimeric antigen receptors-T cells.
References
-
- Rodriguez-Abreu D, Bordoni A, Zucca E. Epidemiology of hematological malignancies. Ann Oncol 2007; 18(Suppl. 1): i3–i8. - PubMed
-
- Chaganti S, Illidge T, Barrington S, et al.. Guidelines for the management of diffuse large B-cell lymphoma. Br J Haematol 2016; 174: 43–56. - PubMed
-
- International Non-Hodgkin’s Lymphoma Prognostic Factors Project. A predictive model for aggressive non-Hodgkin’s lymphoma. N Engl J Med 1993; 329: 987–994. - PubMed
-
- Rosenwald A, Wright G, Chan WC, et al.. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. N Engl J Med 2002; 346: 1937–1947. - PubMed
-
- Alizadeh AA, Eisen MB, Davis RE, et al.. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature 2000; 403: 503–511. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
