

The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study
- PMID: 34733862
- PMCID: PMC8558376
- DOI: 10.3389/fmed.2021.739596
The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study
Abstract
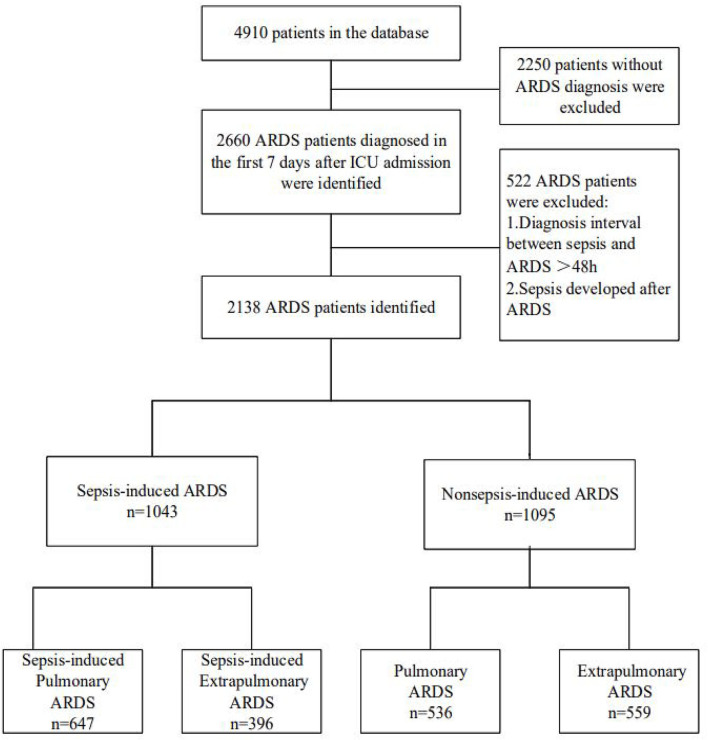
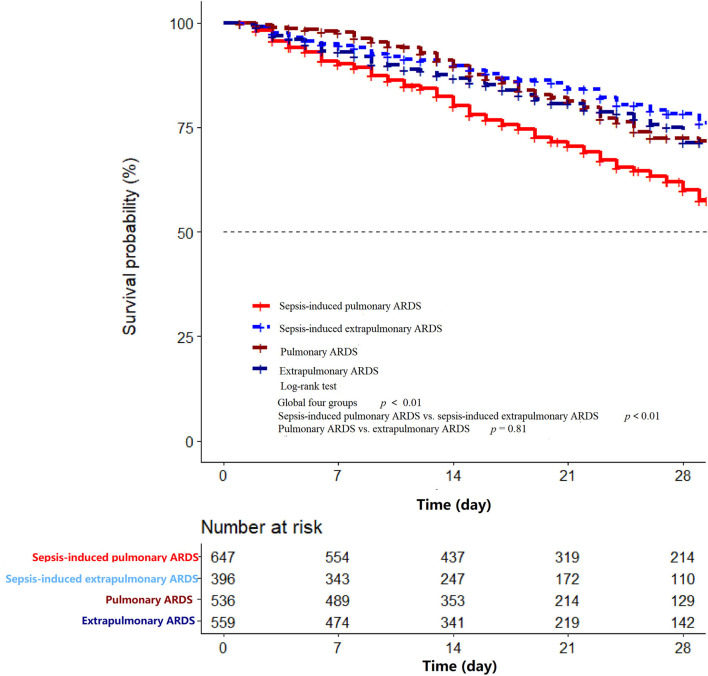
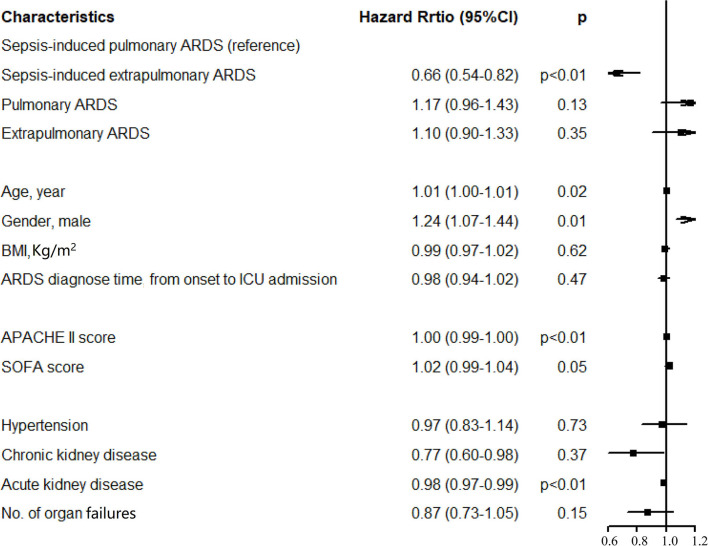
Background: Lung-protective ventilation (LPV) strategies have been beneficial in patients with acute respiratory distress syndrome (ARDS). As a vital part of LPV, positive end-expiratory pressure (PEEP) can enhance oxygenation. However, randomized clinical trials of different PEEP strategies seem to show no advantages in clinical outcomes in patients with ARDS. A potential reason is that diverse etiologies and phenotypes in patients with ARDS may account for different PEEP responses, resulting in variations in mortality. We consider hospital mortality to be associated with a more specific classification of ARDS, such as sepsis induced or not, and pulmonary or extrapulmonary one. Our study aimed to compare clinical outcomes in various patients with ARDS by etiologies using the China Critical Care Sepsis Trial (CCCST) database. This was a retrospective analysis of a prospective cohort of 2,138 patients with ARDS in the CCCST database. According to ARDS induced by sepsis or not and medical history, patients were stratified into different four groups. Differences among groups were assessed in hospital mortality, ventilation-free days, and other clinical features. Results: A total of 2,138 patients with ARDS were identified in the database, including 647 patients with sepsis-induced pulmonary ARDS (30.3%), 396 patients with sepsis-induced extrapulmonary ARDS (18.5%), 536 patients with non-sepsis pulmonary ARDS (25.1%), and 559 patients with non-sepsis extrapulmonary ARDS (26.1%). The pulmonary ARDS group had higher mortality compared with the extrapulmonary group (45.9 vs. 23.0%, p < 0.01), longer intensive care unit (ICU) and hospital stays (9 vs. 6 days, p < 0.01, 20 vs. 18 days, p = 0.01, respectively), and fewer ventilation-free days (5 vs. 9 days) in the presence of sepsis. However, the mortality in ARDS without sepsis was inverted compared with extrapulmonary ARDS (pulmonary 23.5% vs. extrapulmonary 29.2%, p = 0.04). After adjusting for the Acute Physiology and Chronic Health Evaluation II and sequential organ failure assessment scores and other clinical features, the sepsis-induced pulmonary condition was still a risk factor for death in patients with ARDS (hazard ratio 0.66, 95% CI, 0.54-0.82, p < 0.01) compared with sepsis-induced extrapulmonary ARDS and other subphenotypes. Conclusions: In the presence of sepsis, hospital mortality in pulmonary ARDS is higher compared with extrapulmonary ARDS; however, mortality is inverted in ARDS without sepsis. Sepsis-induced pulmonary ARDS should attract more attention from ICU physicians and be cautiously treated. Trial registration: ChiCTR-ECH-13003934. Registered August 3, 2013, http://www.chictr.org.cn.
Keywords: ARDS; clinical outcome; etiology; hospital mortality; pulmonary and extrapulmonary causes.
Copyright © 2021 Wang, Zhang, Xi, Zhou and the China Critical Care Sepsis Trial (CCCST) Workgroup.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials