

Cardiovascular outcomes after cardiac resynchronization therapy in cardiac amyloidosis
- PMID: 34734471
- PMCID: PMC8787999
- DOI: 10.1002/ehf2.13663
Cardiovascular outcomes after cardiac resynchronization therapy in cardiac amyloidosis
Abstract
Aims: Cardiac resynchronization therapy (CRT) is highly effective in dilated cardiomyopathy (DCM) patients with impaired left ventricular ejection fraction (LVEF) and left bundle block branch. In cardiac amyloidosis (CA) patients, left ventricular dysfunction and conduction defects are common, but the potential of CRT to improve cardiac remodelling and survival in this particular setting remains undefined. We investigated cardiovascular outcomes in CA patients after CRT implantation in terms of CRT echocardiographic response and major cardiovascular events (MACEs).
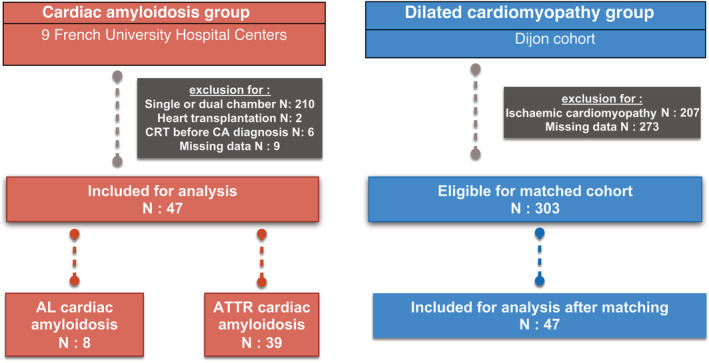
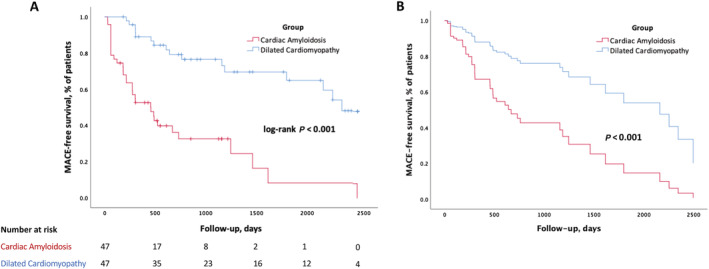
Methods and results: Our retrospective study included 47 CA patients implanted with CRT devices from January 2012 to February 2020, in nine French university hospitals (77 ± 6 years old, baseline LVEF 30 ± 8%) compared with propensity-matched (1:1 for age, LVEF at implantation, and CRT indication) DCM patients with a CRT device. CA patients had lower rates of CRT response (absolute delta LVEF ≥ 10%) compared with DCM patients (36% vs. 70%, P = 0.002). After multivariate Cox analysis, CA was independently associated with MACE (hospitalization for heart failure/cardiovascular death) [hazard ratio (HR) 3.73, 95% confidence interval (CI) 1.85-7.54, P < 0.001], along with the absence of CRT response (HR 3.01, 95% CI 1.56-5.79, P = 0.001). The presence of echocardiographic CRT response (absolute delta LVEF ≥ 10%) was the only predictive factor of MACE-free survival in CA patients (HR 0.36, 95% CI 0.15-0.86, P = 0.002).
Conclusion: Compared with a matched cohort of DCM patients, CA patients had a lower rate of CRT response and consequently a worse cardiovascular prognosis after CRT implantation. However, CRT could be beneficial even in CA patients given that CRT response was associated with better cardiac outcomes in this population.
Keywords: Cardiac amyloidosis; Cardiac resynchronization therapy; Heart failure; Implantable cardioverter defibrillator; Pacemaker.
© 2021 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
T.D. reports grants and personal fees from Pfizer and Ionis‐Akcea and personal fees from Alnylam and Neurimmune, during the conduct of the study. G.L. reports personal fees from Abbott, Biosense Webster, MicroPort CRM, Boston Scientific, Medtronic, and Biotronik, outside the submitted work. C.G. reports personal fees from MicroPort CRM, Boston Scientific, and Medtronic, outside the submitted work. J.‐B.G. reports personal fees from Abbott and non‐financial support from Bayer, outside the submitted work. N.C. reports personal fees from Medtronic, outside the submitted work. F.L. reports non‐financial support from MicroPort and Johnson & Johnson and personal fees from Meda Pharma, Sanofi, Bayer, and Pfizer, outside the submitted work. The other authors have nothing to declare.
Figures
References
-
- Gertz MA, Dispenzieri A, Sher T. Pathophysiology and treatment of cardiac amyloidosis. Nat Rev Cardiol 2015; 12: 91–102. - PubMed
-
- Damy T, Jaccard A, Guellich A, Lavergne D, Galat A, Deux J‐F, Hittinger L, Dupuis J, Frenkel V, Rigaud C, Plante‐Bordeneuve V, Bodez D, Mohty D. Identification of prognostic markers in transthyretin and AL cardiac amyloidosis. Amyloid Int J Exp Clin Investig Off J Int Soc Amyloidosis 2016; 23: 194–202. - PubMed
-
- Algalarrondo V, Dinanian S, Juin C, Chemla D, Bennani SL, Sebag C, Planté V, Le Guludec D, Samuel D, Adams D, Slama MS. Prophylactic pacemaker implantation in familial amyloid polyneuropathy. Heart Rhythm 2012; 9: 1069–1075. - PubMed
-
- Bogale N, Witte K, Priori S, Cleland J, Auricchio A, Gadler F, Gitt A, Limbourg T, Linde C, Dickstein K, the Scientific Committee, National coordinators and the investigators . The European Cardiac Resynchronization Therapy Survey: comparison of outcomes between de novo cardiac resynchronization therapy implantations and upgrades. Eur J Heart Fail 2011; 13: 974–983. - PubMed
-
- Curtis AB, Worley SJ, Chung ES, Li P, Christman SA, St. John Sutton M. Improvement in clinical outcomes with biventricular versus right ventricular pacing: the BLOCK HF study. J Am Coll Cardiol American College of Cardiology Foundation 2016; 67: 2148–2157. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
