

Peripheral intravascular lithotripsy for transcatheter aortic valve implantation: a multicentre observational study
- PMID: 34734559
- PMCID: PMC9896402
- DOI: 10.4244/EIJ-D-21-00581
Peripheral intravascular lithotripsy for transcatheter aortic valve implantation: a multicentre observational study
Abstract
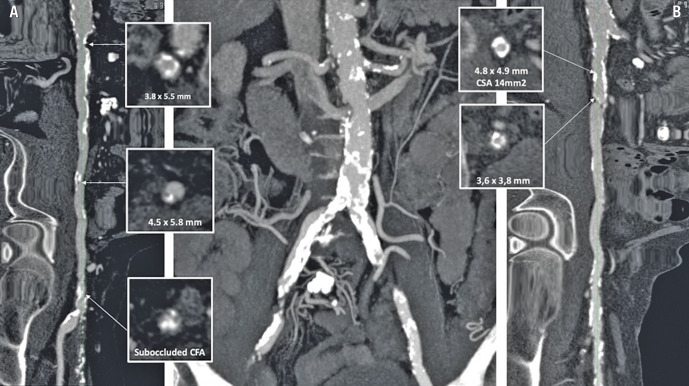
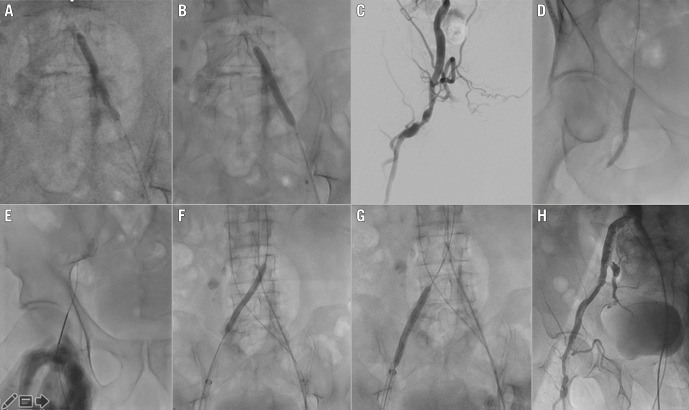
Background: The presence of severe calcific atherosclerosis at the iliofemoral axis may preclude transcatheter aortic valve implantation (TAVI) by the transfemoral (TF) approach. Intravascular lithotripsy (IVL) is a novel technology that fractures intimal/medial calcium and increases vessel compliance allowing TF TAVI in selected patients with peripheral artery disease (PAD).
Aims: The aim of this study was to report on the safety and efficacy of IVL-assisted TF TAVI in an all-comers population.
Methods: Clinical, imaging and procedural data on all consecutive patients treated by IVL-assisted TF TAVI in six high-volume European centres (2018-2020) were collected in this prospective, real-world, multicentre registry.
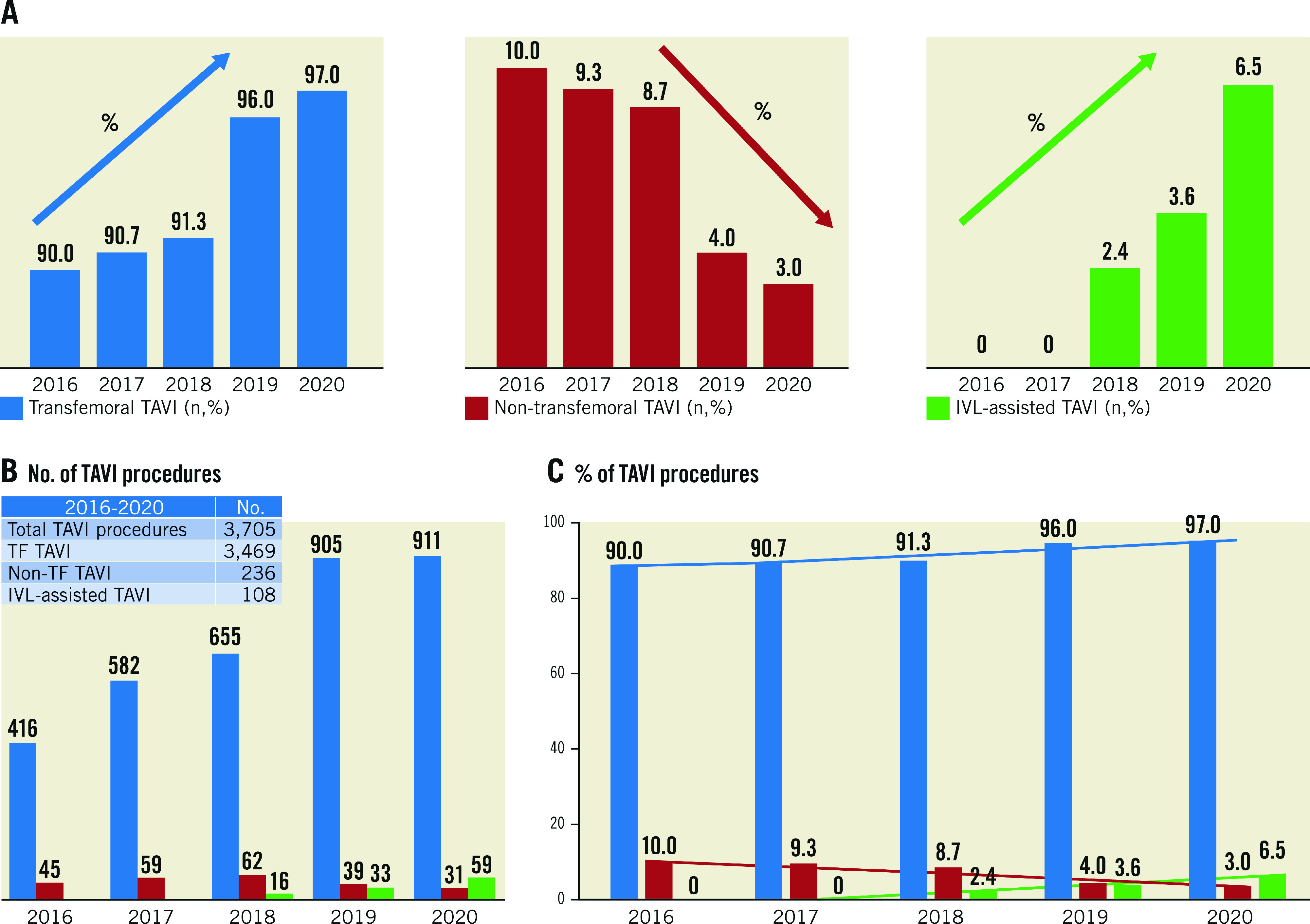
Results: IVL-assisted TF TAVI was performed in 108 patients, increasing from 2.4% to 6.5% of all TAVI from 2018 to 2020, respectively. The target lesion was most often localised at the common and/or external iliac artery (93.5% of cases; average TL-MLD 4.6±0.9 mm with 318 degrees of calcium arc). Transfemoral aortic valve delivery was successful in 100% of cases; final procedural success in 98.2% (two conversions to cardiac open surgery for annular rupture and valve migration). Complications of the IVL-treated segments consisted of 1 perforation and 3 major dissections requiring stent implantation (2 covered stents and 2 BMS). Access-site-related complications included 3 major bleedings. Three in-hospital deaths were recorded (2.8%, 1 failed surgical conversion after annular rupture, 1 cardiac arrest after initial valvuloplasty, 1 late hyperkalaemia in renal dysfunction).
Conclusions: IVL-assisted TF TAVI proved to be a safe and effective approach, which helps to expand the indications for TF TAVI in patients with severe calcific PAD. However, these patients continue to have a higher-than-average incidence of periprocedural complications.
Conflict of interest statement
O. De Backer has received institutional research grants and consulting fees from Abbott, Boston Scientific and Shockwave Medical Inc. O. De Backer has received speaker fees from Shockwave Medical. F. Saia is a member of the Advisory Board for Edwards, Medtronic, Abbott, Bayer, Biotronik, Amgen, Boehringer-Ingelheim, and AstraZeneca, and has received lecture fees from Edwards, Medtronic, Abbott, Bayer, Amgen, Boehringer-Ingelheim, AstraZeneca, Boston Scientific, Volcano, and Chiesi, outside the submitted work. F. Meucci reports receiving speaker and consultation fees from Medtronic, Edwards and Boston Scientific. T. Palmerini has received lecture fees from Biotronik and Edwards. C. Di Mario has received research or educational grants from Abbott, Amgen, Asahi Intecc, AstraZeneca, Boston Scientific, Cardinal Health, CSL Behring, Chiesi, Daiichi Sankyo, Edwards, Medtronic, Menarini, Pfizer, Sanofi, Shockwave, Teleflex, and Volcano/Philips. The other authors have no conflicts of interest to declare. The Guest Editor reports lecture fees paid to his institution from Amgen, Bayer Healthcare, Biotronik, Boehringer Ingelheim, Boston Scientific, Daiichi Sankyo, Edwards Lifesciences, Ferrer, Pfizer, and Novartis, consultancy fees paid to his institution from Boehringer Ingelheim, and grant support from Bayer Healthcare, Boston Scientific, Biotronik, Edwards Lifesciences, GlaxoSmithKline, Medtronic, and Pfizer.
Figures
References
-
- Patel JS, Krishnaswamy A, Svensson LG, Tuzcu EM, Mick S, Kapadia SR. Access Options for Transcatheter Aortic Valve Replacement in Patients with Unfavorable Aortoiliofemoral Anatomy. Curr Cardiol Rep. 2016;18:110. - PubMed
-
- Kurra V, Schoenhagen P, Roselli EE, Kapadia SR, Tuzcu EM, Greenberg R, Akhtar M, Desai MY, Flamm SD, Halliburton SS, Svensson LG, Sola S. Prevalence of significant peripheral artery disease in patients evaluated for percutaneous aortic valve insertion: Preprocedural assessment with multidetector computed tomography. J Thorac Cardiovasc Surg. 2009;137:1258–64. - PubMed
-
- Arai T, Romano M, Lefèvre T, Hovasse T, Farge A, Le Houerou, Hayashida K, Watanabe Y, Garot P, Benamer H, Unterseeh T, Bouvier E, Morice MC, Chevalier B. Direct Comparison of Feasibility and Safety of Transfemoral Versus Transaortic Versus Transapical Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2016;9:2320–5. - PubMed
-
- Guedeney P, Mehran R. Non-femoral TAVR: Time to stratify alternative vascular approaches. Catheter Cardiovasc Interv. 2018;92:1194–5. - PubMed
-
- Brodmann M, Werner M, Holden A, Tepe G, Scheinert D, Schwindt A, Wolf F, Jaff M, Lansky A, Zeller T. Primary outcomes and mechanism of action of intravascular lithotripsy in calcified, femoropopliteal lesions: Results of Disrupt PAD II. Catheter Cardiovasc Interv. 2019;93:335–42. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous