

Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity
- PMID: 34734975
- PMCID: PMC8569602
- DOI: 10.1001/jama.2021.19499
Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity
Abstract
Importance: A comprehensive understanding of the benefits of COVID-19 vaccination requires consideration of disease attenuation, determined as whether people who develop COVID-19 despite vaccination have lower disease severity than unvaccinated people.
Objective: To evaluate the association between vaccination with mRNA COVID-19 vaccines-mRNA-1273 (Moderna) and BNT162b2 (Pfizer-BioNTech)-and COVID-19 hospitalization, and, among patients hospitalized with COVID-19, the association with progression to critical disease.
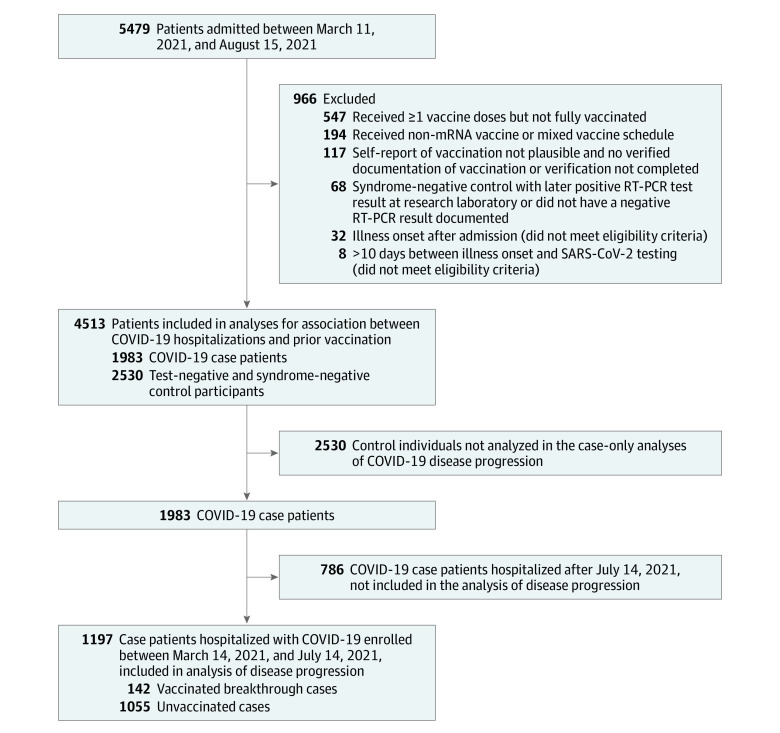
Design, setting, and participants: A US 21-site case-control analysis of 4513 adults hospitalized between March 11 and August 15, 2021, with 28-day outcome data on death and mechanical ventilation available for patients enrolled through July 14, 2021. Date of final follow-up was August 8, 2021.
Exposures: COVID-19 vaccination.
Main outcomes and measures: Associations were evaluated between prior vaccination and (1) hospitalization for COVID-19, in which case patients were those hospitalized for COVID-19 and control patients were those hospitalized for an alternative diagnosis; and (2) disease progression among patients hospitalized for COVID-19, in which cases and controls were COVID-19 patients with and without progression to death or mechanical ventilation, respectively. Associations were measured with multivariable logistic regression.
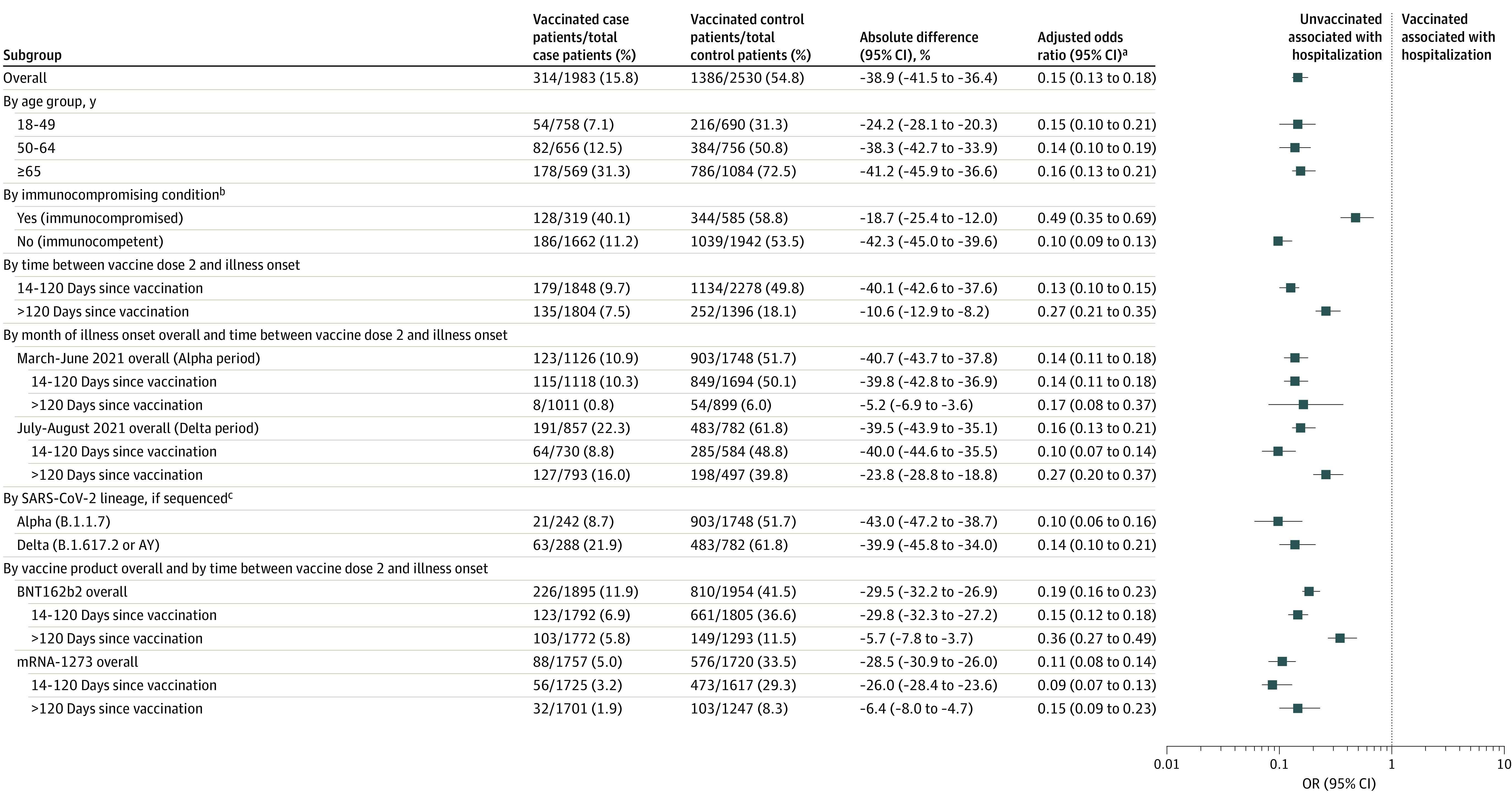
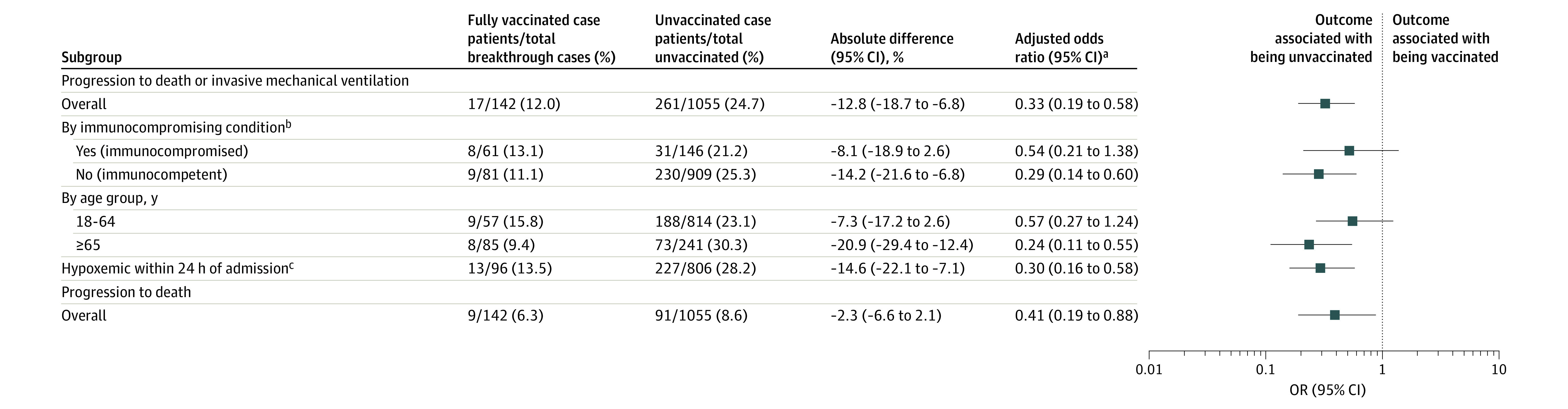
Results: Among 4513 patients (median age, 59 years [IQR, 45-69]; 2202 [48.8%] women; 23.0% non-Hispanic Black individuals, 15.9% Hispanic individuals, and 20.1% with an immunocompromising condition), 1983 were case patients with COVID-19 and 2530 were controls without COVID-19. Unvaccinated patients accounted for 84.2% (1669/1983) of COVID-19 hospitalizations. Hospitalization for COVID-19 was significantly associated with decreased likelihood of vaccination (cases, 15.8%; controls, 54.8%; adjusted OR, 0.15; 95% CI, 0.13-0.18), including for sequenced SARS-CoV-2 Alpha (8.7% vs 51.7%; aOR, 0.10; 95% CI, 0.06-0.16) and Delta variants (21.9% vs 61.8%; aOR, 0.14; 95% CI, 0.10-0.21). This association was stronger for immunocompetent patients (11.2% vs 53.5%; aOR, 0.10; 95% CI, 0.09-0.13) than immunocompromised patients (40.1% vs 58.8%; aOR, 0.49; 95% CI, 0.35-0.69) (P < .001) and weaker at more than 120 days since vaccination with BNT162b2 (5.8% vs 11.5%; aOR, 0.36; 95% CI, 0.27-0.49) than with mRNA-1273 (1.9% vs 8.3%; aOR, 0.15; 95% CI, 0.09-0.23) (P < .001). Among 1197 patients hospitalized with COVID-19, death or invasive mechanical ventilation by day 28 was associated with decreased likelihood of vaccination (12.0% vs 24.7%; aOR, 0.33; 95% CI, 0.19-0.58).
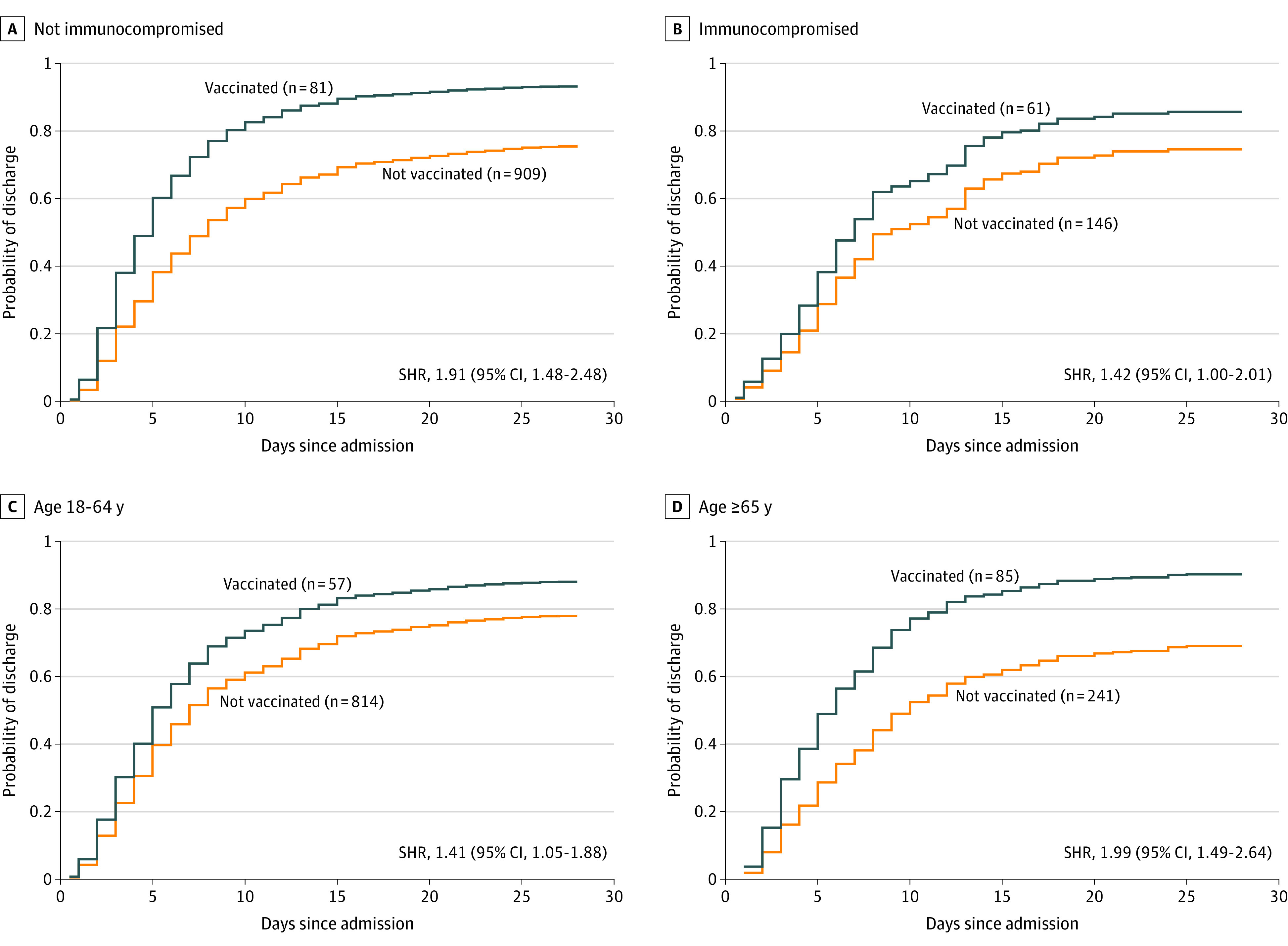
Conclusions and relevance: Vaccination with an mRNA COVID-19 vaccine was significantly less likely among patients with COVID-19 hospitalization and disease progression to death or mechanical ventilation. These findings are consistent with risk reduction among vaccine breakthrough infections compared with absence of vaccination.
Conflict of interest statement
Figures
Comment in
-
Understanding Breakthrough Infections Following mRNA SARS-CoV-2 Vaccination.JAMA. 2021 Nov 23;326(20):2018-2020. doi: 10.1001/jama.2021.19063. JAMA. 2021. PMID: 34734985 No abstract available.
References
-
- Haas EJ, Angulo FJ, McLaughlin JM, et al. . Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: an observational study using national surveillance data. Lancet. 2021;397(10287):1819-1829. doi:10.1016/S0140-6736(21)00947-8 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
