

Accessibility of Pharmacist-Prescribed Contraceptives in Utah
- PMID: 34735383
- PMCID: PMC8594517
- DOI: 10.1097/AOG.0000000000004594
Accessibility of Pharmacist-Prescribed Contraceptives in Utah
Abstract
Objective: To assess pharmacy participation in and accessibility of pharmacist-prescribed contraception after legislation effective in the state of Utah in 2019.
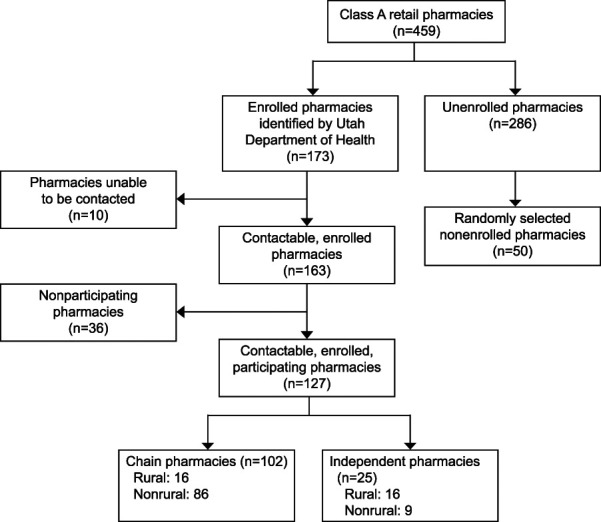
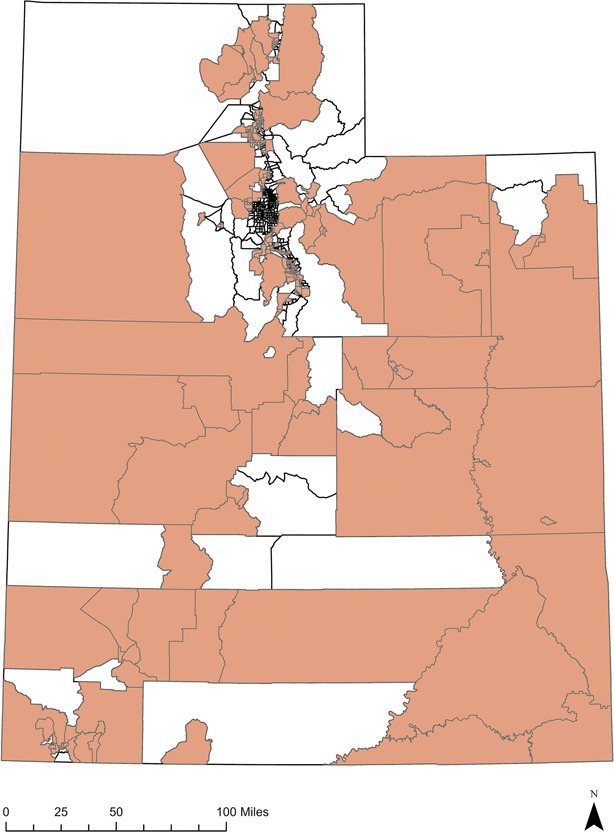
Methods: A secret-shopper telephone survey was used to assess participation in pharmacist-prescribed contraception. Geospatial analysis was used to map the distribution of participating pharmacies by population characteristics.
Results: Of all operating Class A retail pharmacies in Utah, 127 (27%) were providing pharmacist-prescribed contraception 1 year after implementation of the Utah standing order. Oral contraceptive pills were widely accessible (100%); however, other allowed methods were not (vaginal ring 14%; contraceptive patch 2%). Consultation fees and medication costs varied widely. Participating pharmacies were mainly concentrated in population centers. Assuming access to a personal vehicle, urban areas with a high percentage of Hispanic people (Utah's largest minority race or ethnicity group) have access to a participating pharmacy within a 20-minute driving distance. However, access in rural areas with a high percentage Hispanic or other minority were limited. We identified 235 (40%) census tracts with a high proportion of Utah's residents living below the poverty line or of minority race or ethnicity who also had low access to pharmacist-prescribed contraception.
Conclusions: Although the pharmacy-based model is intended to increase access to contraception, practical availability 1 year after the authorization of pharmacist-prescribed contraception in Utah suggests that this service does not adequately serve rural areas, particularly rural areas with a high proportion of minorities and those living below the federal poverty line.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Financial Disclosure The authors did not report any potential conflicts of interest.
Figures
References
-
- Jones J, Mosher W, Daniels K. Current contraceptive use in the United States 2006-2010, and changes in patterns of use since 1995. Natl Health Stat Rep 2012:1–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
