

Early childhood height-adjusted total kidney volume as a risk marker of kidney survival in ARPKD
- PMID: 34737334
- PMCID: PMC8568977
- DOI: 10.1038/s41598-021-00523-z
Early childhood height-adjusted total kidney volume as a risk marker of kidney survival in ARPKD
Abstract
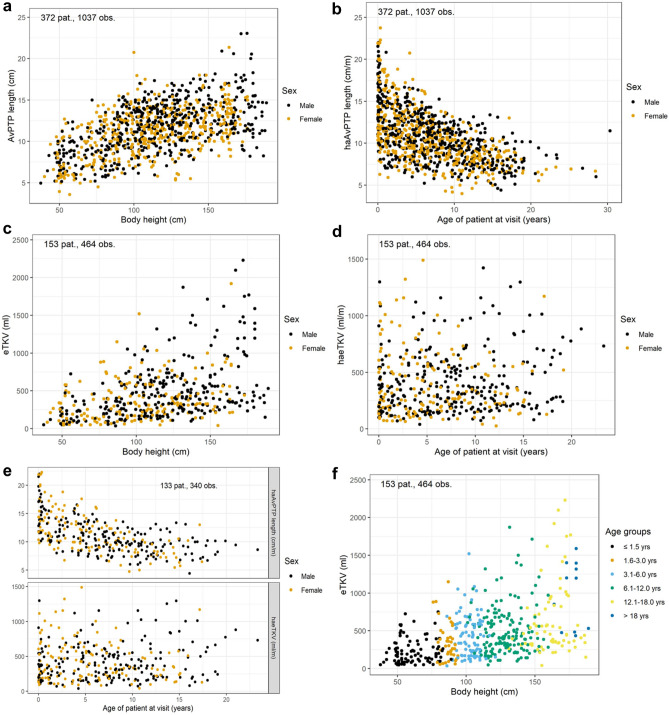
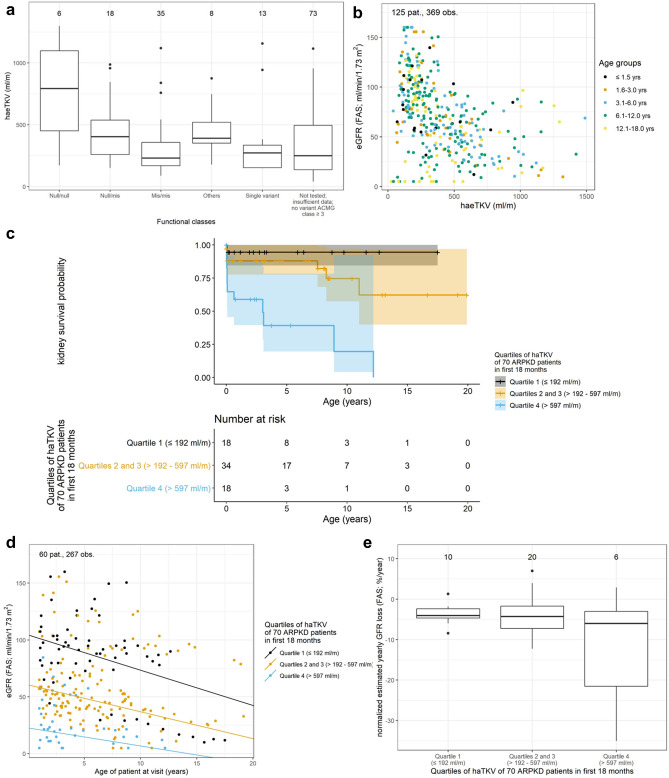
Autosomal recessive polycystic kidney disease (ARPKD) is characterized by bilateral fibrocystic changes resulting in pronounced kidney enlargement. Impairment of kidney function is highly variable and widely available prognostic markers are urgently needed as a base for clinical decision-making and future clinical trials. In this observational study we analyzed the longitudinal development of sonographic kidney measurements in a cohort of 456 ARPKD patients from the international registry study ARegPKD. We furthermore evaluated correlations of sonomorphometric findings and functional kidney disease with the aim to describe the natural disease course and to identify potential prognostic markers. Kidney pole-to-pole (PTP) length and estimated total kidney volume (eTKV) increase with growth throughout childhood and adolescence despite individual variability. Height-adjusted PTP length decreases over time, but such a trend cannot be seen for height-adjusted eTKV (haeTKV) where we even observed a slight mean linear increase of 4.5 ml/m per year during childhood and adolescence for the overall cohort. Patients with two null PKHD1 variants had larger first documented haeTKV values than children with missense variants (median (IQR) haeTKV 793 (450-1098) ml/m in Null/null, 403 (260-538) ml/m in Null/mis, 230 (169-357) ml/m in Mis/mis). In the overall cohort, estimated glomerular filtration rate decreases with increasing haeTKV (median (IQR) haeTKV 210 (150-267) ml/m in CKD stage 1, 472 (266-880) ml/m in stage 5 without kidney replacement therapy). Strikingly, there is a clear correlation between haeTKV in the first eighteen months of life and kidney survival in childhood and adolescence with ten-year kidney survival rates ranging from 20% in patients of the highest to 94% in the lowest quartile. Early childhood haeTKV may become an easily obtainable prognostic marker of kidney disease in ARPKD, e.g. for the identification of patients for clinical studies.
© 2021. The Author(s).
Conflict of interest statement
Dr. Liebau has received honoraria for scientific lectures from Pfizer. Representing the University Hospital of Cologne, Dr. Liebau has been counselling Otsuka in an advisory board. Dr. Mekahli, represented by KU Leuven University, received an educational grant from Otsuka and participated in an advisory board. The other authors declare no potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
