Endoscopic Keyhole Approach for Intracranial Epidermoid
- PMID: 34737493
- PMCID: PMC8559065
- DOI: 10.1055/s-0041-1735283
Endoscopic Keyhole Approach for Intracranial Epidermoid
Abstract
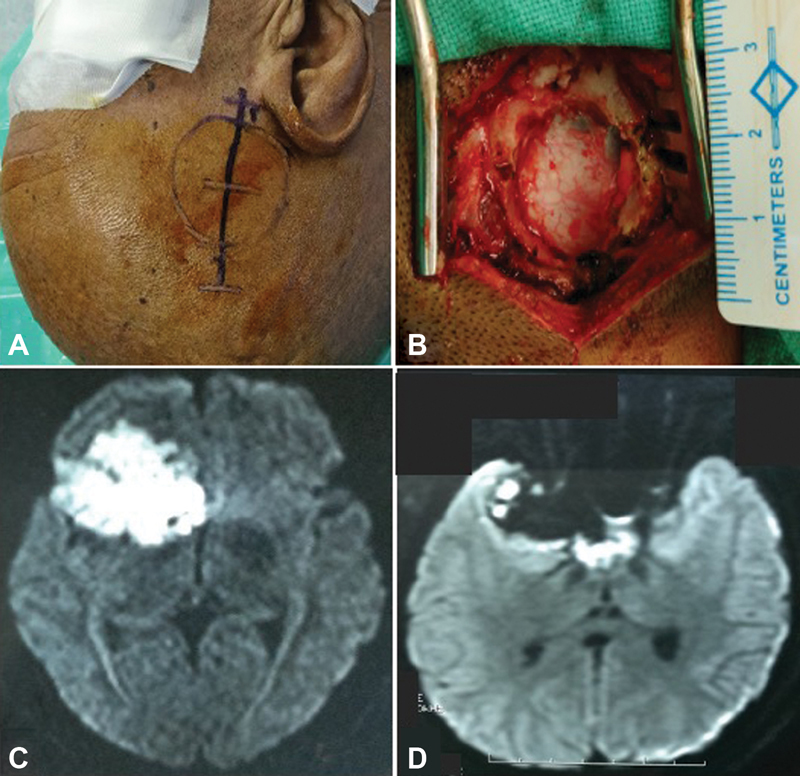
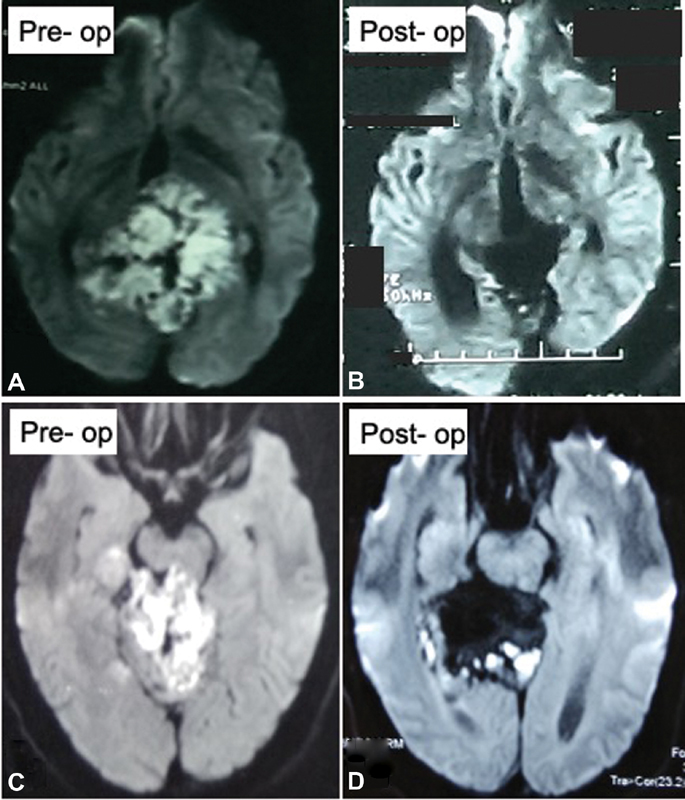
Objective In contemporary neurosurgical practice, keyhole endoscopic approach has established its role in various neurosurgical pathologies. Intracranial epidermoid is an ideal pathology for endoscopic keyhole approach as epidermoid is well encapsulated, extra-axial, avascular, and easily suckable. The objective of this study is to share our experience of endoscopic keyhole approach for intracranial epidermoids at various locations as a new minimally invasive neurosurgical approach to deal with these lesions. Materials and Methods We conducted a retrospective study on 26 patients who underwent keyhole pure endoscopic excision of intracranial epidermoid between July 2015 and December 2019. Patient's demographics, clinical features, radiological imaging, and postoperative complications were noted. Follow-up outcome of preoperative symptoms and postoperative complications were also analyzed. Results The mean age of the study population was 30.5 years with a mean follow-up of 30 months. The common presenting features were headache, hearing loss, and trigeminal neuralgic pain. Gross total resection was achieved in 73.1% cases, while near total resection and subtotal resection were achieved in 19.2 and 7.7% cases, respectively. In the follow-up, maximal improvement was seen in trigeminal neuralgic pain (83%) and headache (66.7%). Major postoperative complications were facial nerve paresis, lower cranial nerve paresis, and transient facial hypoesthesia, most of which improved over time. None of the patients required resurgery till date. Statistical Analysis Patients' data were analyzed using SPSS software version 23 (Statistical Package for Social Sciences, IBM, Chicago, United States). Conclusion This study demonstrates that with careful patient selection, endoscopic keyhole excision of epidermoid is a good alternative to conventional microsurgical excision with comparable surgical and functional outcomes.
Keywords: endoscopic; epidermoid; intracranial; keyhole; minimally invasive techniques; pure; tailored craniotomy.
Association for Helping Neurosurgical Sick People. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures







References
-
- Hoshide R, Faulkner H, Teo M, Teo C. Keyhole retrosigmoid approach for large vestibular schwannomas: strategies to improve outcomes. Neurosurg Focus. 2018;44(03):E2. - PubMed
-
- Sughrue M E, Othman J, Mills S A, Bonney P A, Maurer A J, Teo C. Keyhole transsylvian resection of infiltrative insular gliomas: technique and anatomic results. Turk Neurosurg. 2016;26(04):475–483. - PubMed
-
- Kobata H, Kondo A, Iwasaki K.Cerebellopontine angle epidermoids presenting with cranial nerve hyperactive dysfunction: pathogenesis and long-term surgical results in 30 patients Neurosurgery 20025002276–285., discussion 285–286 - PubMed
-
- Mohanty A, Venkatrama S K, Rao B R, Chandramouli B A, Jayakumar P N, Das B S.Experience with cerebellopontine angle epidermoids Neurosurgery 1997400124–29., discussion 29–30 - PubMed