

How much abdominal fat do obese patients lose short term after laparoscopic sleeve gastrectomy? A quantitative study evaluated with MRI
- PMID: 34737924
- PMCID: PMC8511735
- DOI: 10.21037/qims-20-1380
How much abdominal fat do obese patients lose short term after laparoscopic sleeve gastrectomy? A quantitative study evaluated with MRI
Abstract
Background: This study aimed to elucidate the changes in the amount of abdominal adipose tissue after laparoscopic sleeve gastrectomy in obese Chinese patients over a relatively short follow-up period and to analyze the differences in the effects of surgery between genders.
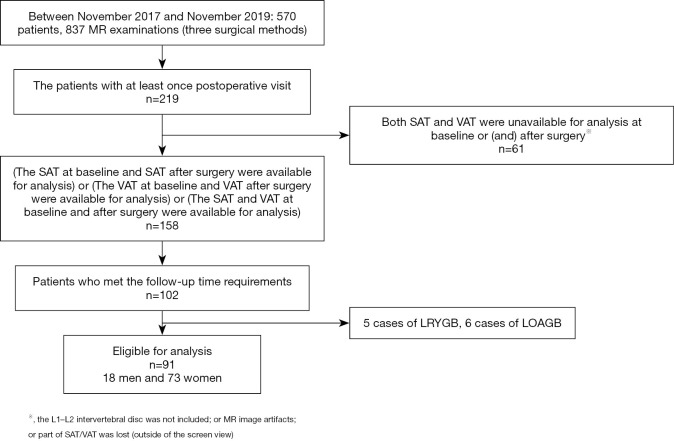
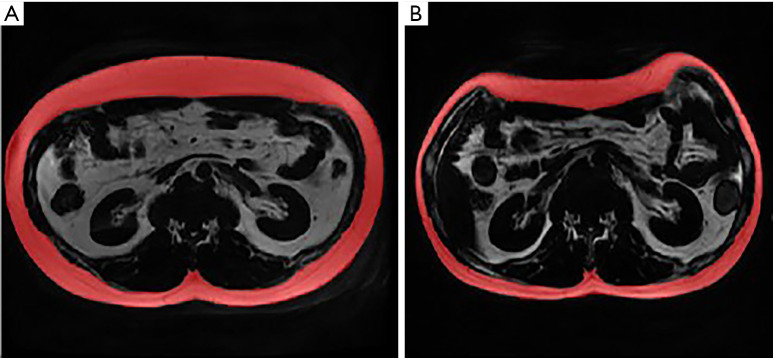
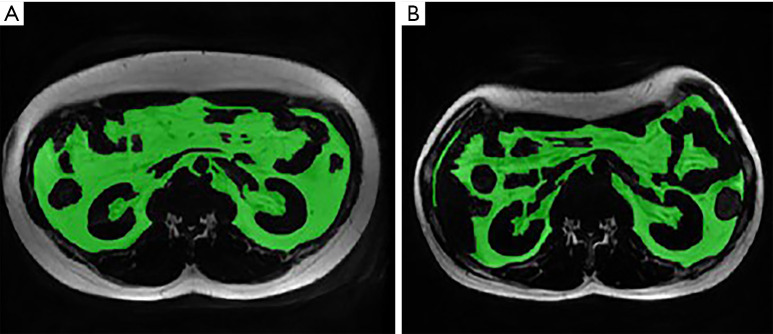
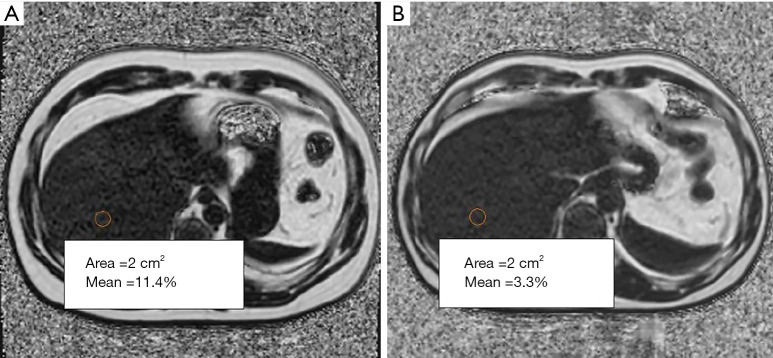
Methods: Ninety-one patients were enrolled in the study, including 18 males and 73 females. These patients underwent laparoscopic sleeve gastrectomy between November 2017 and November 2019. Before and short term after surgery, the areas of subcutaneous/visceral adipose tissue and the liver proton density fat fraction were calculated with upper abdominal magnetic resonance (MR) examinations.
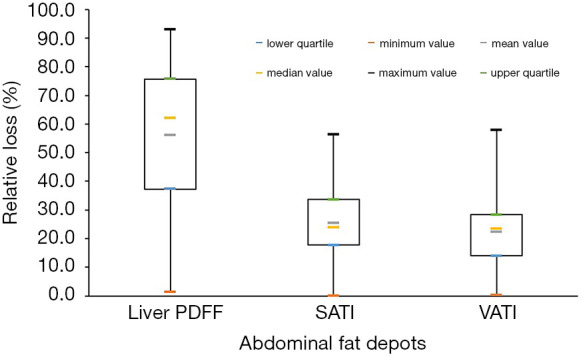
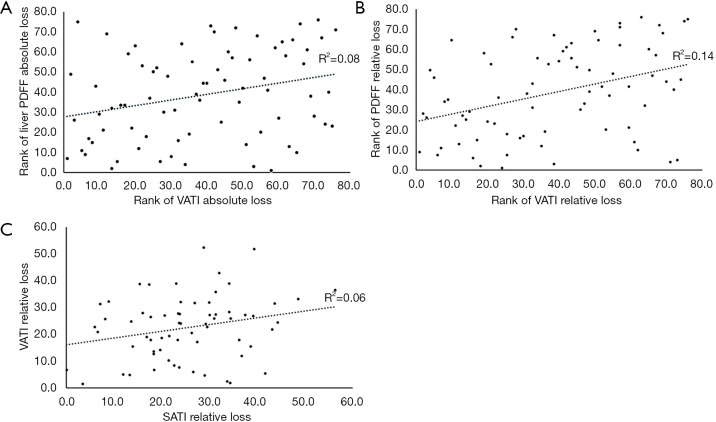
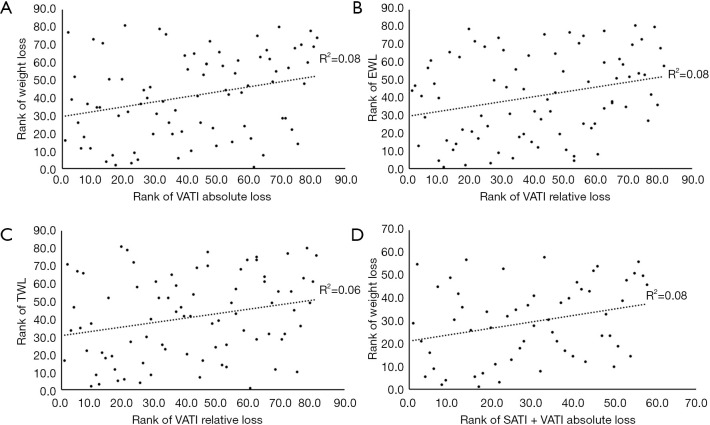
Results: Approximately 100 days after surgery, the median values of weight loss and body mass index reduction were 23.1 kg and 8.1 kg/m2, respectively. The patients achieved a greater absolute loss of subcutaneous adipose tissue index than of visceral adipose tissue index (3.2×10-3 vs. 1.6×10-3, P<0.001). The amount of weight loss, body mass index loss and absolute/relative reduction in visceral adipose tissue index were much greater in males than in females (31.7 vs. 21.7 kg, P<0.001; 9.8 vs. 7.9 kg/m2, P=0.016; 2.5×10-3 vs. 1.3×10-3, P=0.007; 28.2% vs. 20.9%, P=0.029). There was a correlation between decreased amounts in subcutaneous and visceral adipose tissue in sum and weight loss (r=0.282, P=0.032). The absolute/relative reduction in visceral adipose tissue index was also correlated with absolute/relative reduction in liver proton density fat fraction (r=0.283, P=0.013; r=0.372, P=0.001).
Conclusions: The reductions in body weight and visceral fat were more significant in male patients. The sum of absolute reduction in subcutaneous and visceral fat deposits was correlated with weight loss, in all patients enrolled. For severely obese patients, an upper abdominal MR examination could assess the body tissue composition and how it changes after bariatric surgery.
Keywords: Upper abdominal magnetic resonance imaging (upper abdominal MRI); abdominal adipose tissue; bariatric surgery; single magnetic resonance slice (single MR slice).
2021 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/qims-20-1380). The authors have no conflicts of interest to declare.
Figures
References
-
- Lee S, Deldin AR, White D, Kim Y, Libman I, Rivera-Vega M, Kuk JL, Sandoval S, Boesch C, Arslanian S. Aerobic exercise but not resistance exercise reduces intrahepatic lipid content and visceral fat and improves insulin sensitivity in obese adolescent girls: a randomized controlled trial. Am J Physiol Endocrinol Metab 2013;305:E1222-9. 10.1152/ajpendo.00285.2013 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources