

Microvascular Dysfunction in Patients With Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve
- PMID: 34738020
- PMCID: PMC8562107
- DOI: 10.3389/fcvm.2021.765071
Microvascular Dysfunction in Patients With Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve
Abstract
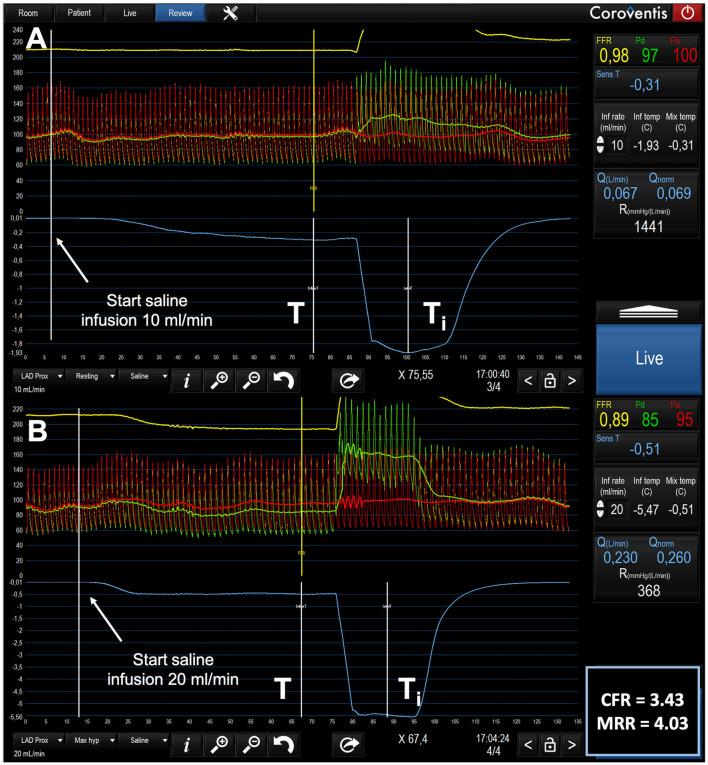
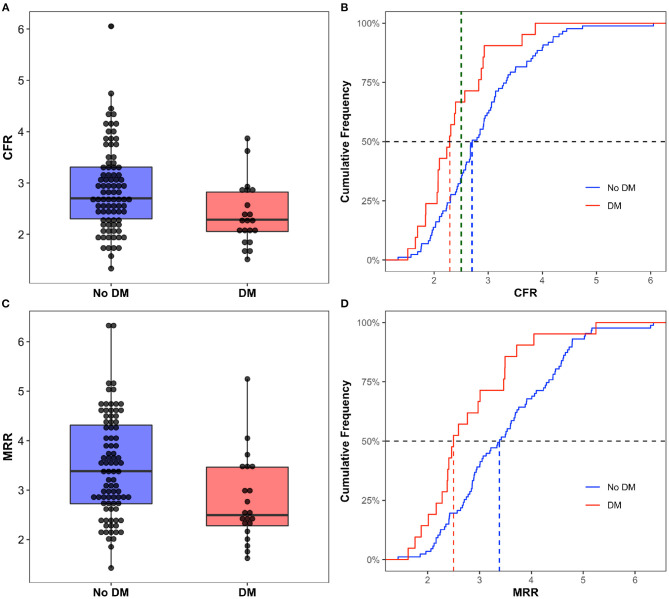
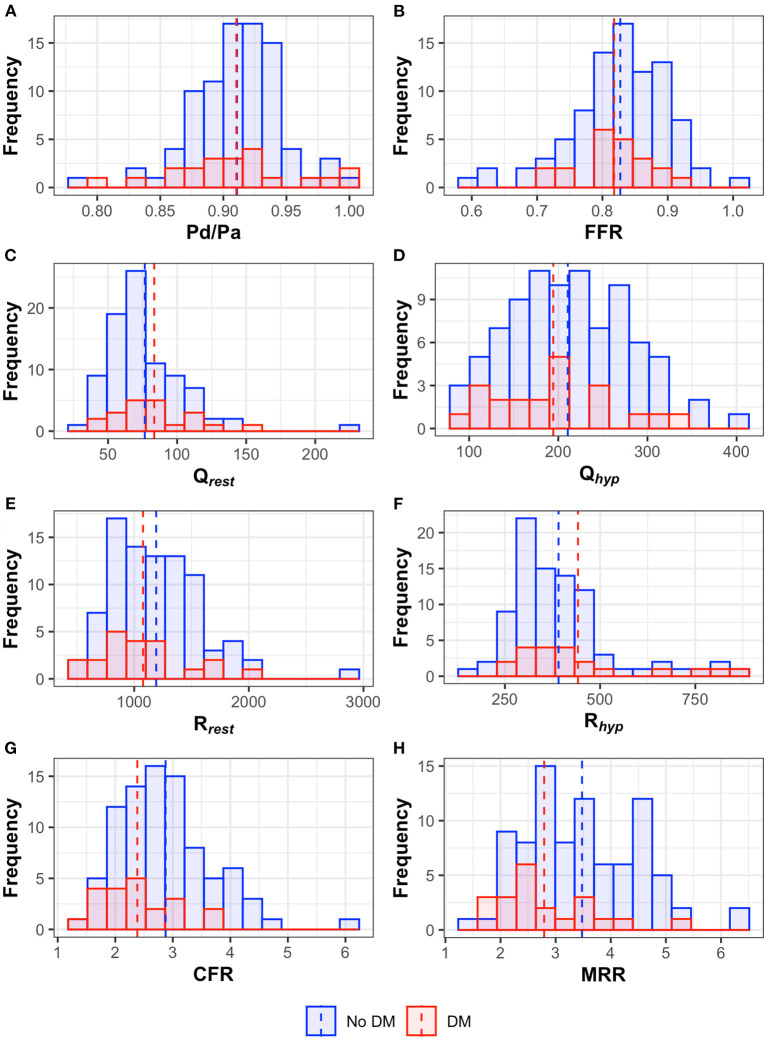
Background: Coronary microvascular dysfunction (CMD) is an early feature of diabetic cardiomyopathy, which usually precedes the onset of diastolic and systolic dysfunction. Continuous intracoronary thermodilution allows an accurate and reproducible assessment of absolute coronary blood flow and microvascular resistance thus allowing the evaluation of coronary flow reserve (CFR) and Microvascular Resistance Reserve (MRR), a novel index specific for microvascular function, which is independent from the myocardial mass. In the present study we compared absolute coronary flow and resistance, CFR and MRR assessed by continuous intracoronary thermodilution in diabetic vs. non-diabetic patients. Left atrial reservoir strain (LASr), an early marker of diastolic dysfunction was compared between the two groups. Methods: In this observational retrospective study, 108 patients with suspected angina and non-obstructive coronary artery disease (NOCAD) consecutively undergoing elective coronary angiography (CAG) from September 2018 to June 2021 were enrolled. The invasive functional assessment of microvascular function was performed in the left anterior descending artery (LAD) with intracoronary continuous thermodilution. Patients were classified according to the presence of DM. Absolute resting and hyperemic coronary blood flow (in mL/min) and resistance (in WU) were compared between the two cohorts. FFR was measured to assess coronary epicardial lesions, while CFR and MRR were calculated to assess microvascular function. LAS, assessed by speckle tracking echocardiography, was used to detect early myocardial structural changes potentially associated with microvascular dysfunction. Results: The median FFR value was 0.83 [0.79-0.87] without any significant difference between the two groups. Absolute resting and hyperemic flow in the left anterior descending coronary were similar between diabetic and non-diabetic patients. Similarly, resting and hyperemic resistances did not change significantly between the two groups. In the DM cohort the CFR and MRR were significantly lower compared to the control group (CFR = 2.38 ± 0.61 and 2.88 ± 0.82; MRR = 2.79 ± 0.87 and 3.48 ± 1.02 for diabetic and non-diabetic patients respectively, [p < 0.05 for both]). Likewise, diabetic patients had a significantly lower reservoir, contractile and conductive LAS (all p < 0.05). Conclusions: Compared with non-diabetic patients, CFR and MRR were lower in patients with DM and non-obstructive epicardial coronary arteries, while both resting and hyperemic coronary flow and resistance were similar. LASr was lower in diabetic patients, confirming the presence of a subclinical diastolic dysfunction associated to the microcirculatory impairment. Continuous intracoronary thermodilution-derived indexes provide a reliable and operator-independent assessment of coronary macro- and microvasculature and might potentially facilitate widespread clinical adoption of invasive physiologic assessment of suspected microvascular disease.
Keywords: continuous thermodilution technique; coronary flow reserve (CFR); coronary microvascular dysfunction (CMD); diabetes mellitus; microcirculatory resistance.
Copyright © 2021 Gallinoro, Paolisso, Candreva, Bermpeis, Fabbricatore, Esposito, Bertolone, Fernandez Peregrina, Munhoz, Mileva, Penicka, Bartunek, Vanderheyden, Wyffels, Sonck, Collet, De Bruyne and Barbato.
Conflict of interest statement
CC reports receiving research grants from Biosensor, Coroventis Research, GE Healthcare, Medis Medical Imaging, Pie Medical Imaging, Cathworks, Boston Scientific, Siemens, HeartFlow Inc. and Abbott Vascular; and consultancy fees from Heart Flow Inc, Opsens, Pie Medical Imaging, Abbott Vascular and Philips Volcano. BD has a consulting relationship with Boston Scientific, Abbott Vascular, CathWorks, Siemens, and Coroventis Research; receives research grants from Abbott Vascular, Coroventis Research, Cathworks, Boston Scientific; and holds minor equities in Philips-Volcano, Siemens, GE Healthcare, Edwards Life Sciences, HeartFlow, Opsens, and Celiad. EB declares speaker's fees from Abbott Vascular, Boston Scientific and GE. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources