

Occurrence of SARS-CoV-2 infection among healthcare personnel: results from an early systematic review and meta-analysis
- PMID: 34738585
- PMCID: PMC8689308
- DOI: 10.23750/abm.v92i5.10438
Occurrence of SARS-CoV-2 infection among healthcare personnel: results from an early systematic review and meta-analysis
Abstract
Background: SARS-CoV-2 infection has become a global public health concern globally. Even though Healthcare Workers (HCWs) are supposedly at increased risk for SARS-CoV-2 infection, to date no pooled evidence has been collected.
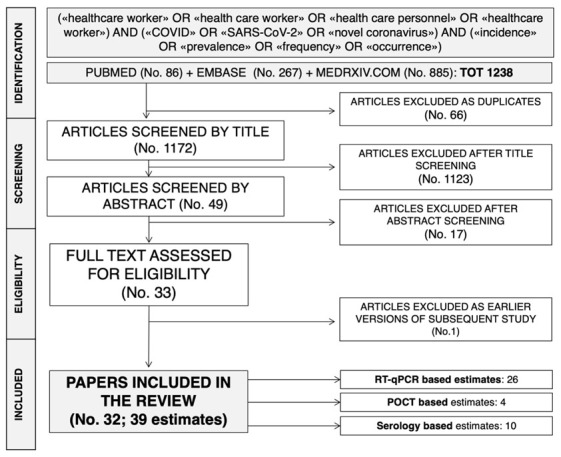
Materials and methods: We searched online electronic databases (PubMed, Embase, medRxiv.org for pre-prints) for all available contribution (up to May 20, 2019). Two Authors independently screened articles and extracted the data. The pooled prevalence of SARS-CoV-2 was analyzed using the random-effects model. The possible sources of heterogeneity were analyzed through subgroup analysis, and meta-regression.
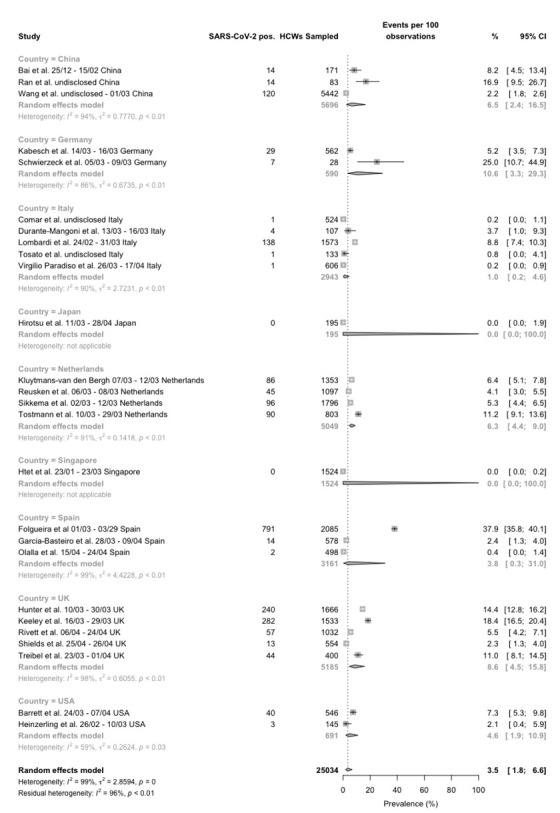
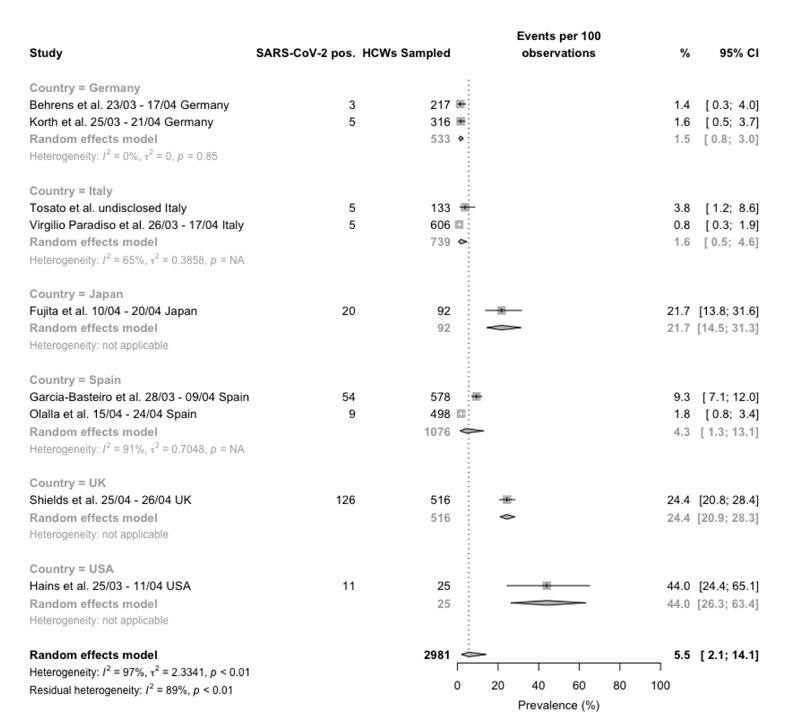
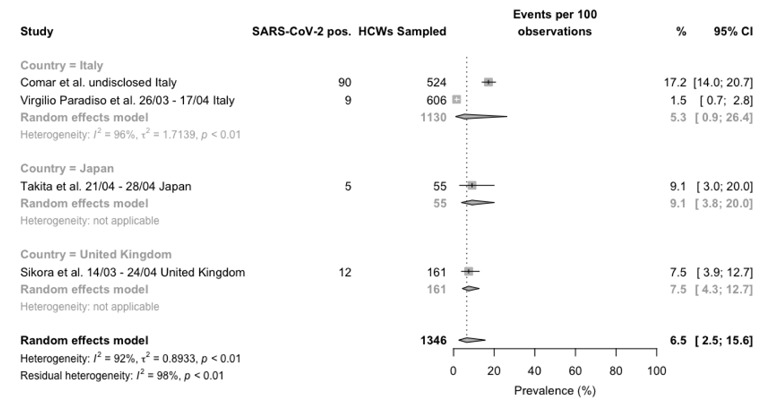
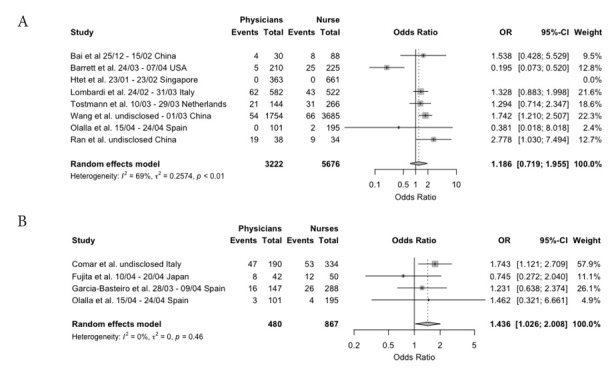
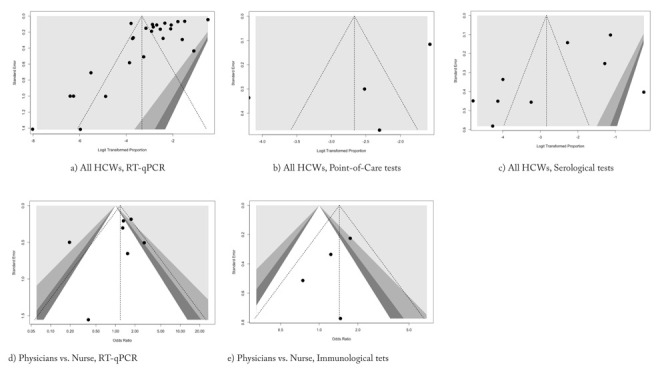
Results: The overall pooled prevalence of SARS-CoV-2 was 3.5% (95%CI 1.8-6.6) for studies based on molecular assays, 5.5% (95%CI 2.1-14.1) for studies based on serological assays, and 6.5% (95%CI 2.5-15.6) for point-of-care capillary blood tests. Among subgroups, serological tests identified higher risk for SARS-CoV-2 seropositivity in physicians than in nurses (OR 1.436, 95%CI 1.026 to 2.008). Regression analysis indicated the possible presence of publication bias only for molecular tests (t -3.3526, p-value 0.002648).
Conclusions: The overall pooled prevalence of SARS-CoV-2 was lower than previously expected, but available studies were affected by significant heterogeneity, and the molecular studies by significant publication bias. Therefore, further high-quality research in the field is warranted.
Conflict of interest statement
The authors declare no conflict of interest. The facts, conclusions, and opinions stated in the article represent the authors’ research, conclusions, and opinions and are believed to be substantiated, accurate, valid, and reliable. However, as this article includes the results of personal researches of the Authors, presenting correspondent, personal conclusions and opinions, parent employers are not forced in any way to endorse or share its content and its potential implications.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
