

Accuracy of Physician Estimates of Out-of-Pocket Costs for Medication Filling
- PMID: 34739059
- PMCID: PMC8571653
- DOI: 10.1001/jamanetworkopen.2021.33188
Accuracy of Physician Estimates of Out-of-Pocket Costs for Medication Filling
Abstract
Importance: One-third of US residents have trouble paying their medical bills. They often turn to their physicians for help navigating health costs and insurance coverage.
Objective: To determine whether physicians can accurately estimate out-of-pocket expenses when they are given all of the necessary information about a drug's price and a patient's insurance plan.
Design, setting, and participants: This national mail-in survey used a random sample of US physicians. The survey was sent to 900 outpatient physicians (300 each of primary care, gastroenterology, and rheumatology). Physicians were excluded if they were in training, worked primarily for the Veterans Administration or Indian Health Service, were retired, or reported 0% outpatient clinical effort. Analyses were performed from July to December 2020.
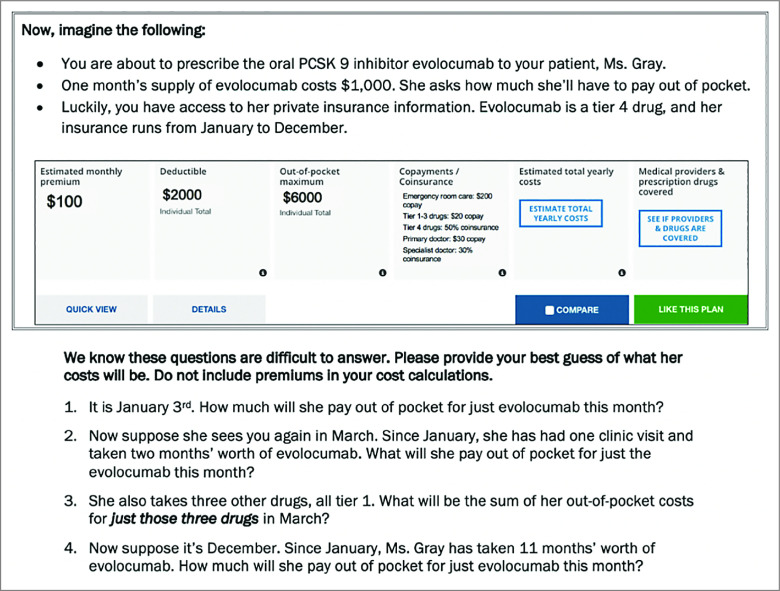
Main outcomes and measures: In a hypothetical vignette, a patient was prescribed a new drug costing $1000/month without insurance. A summary of her private insurance information was provided, including the plan's deductible, coinsurance rates, copays, and out-of-pocket maximum. Physicians were asked to estimate the drug's out-of-pocket cost at 4 time points between January and December, using the plan's 4 types of cost-sharing: (1) deductibles, (2) coinsurance, (3) copays, and (4) out-of-pocket maximums. Multivariate linear regression was used to assess differences in performance by specialty, adjusting for attitudes toward cost conversations, demographics, and clinical characteristics.
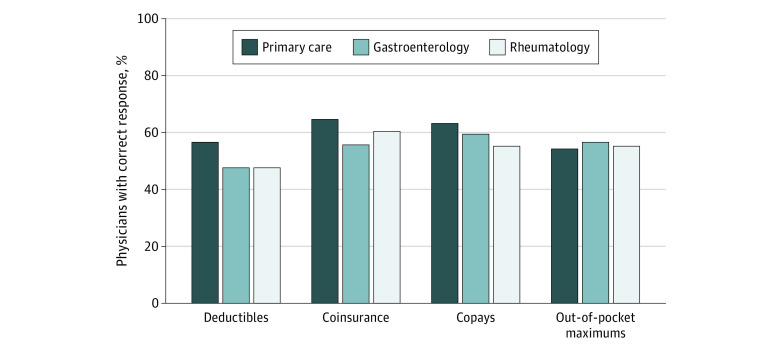
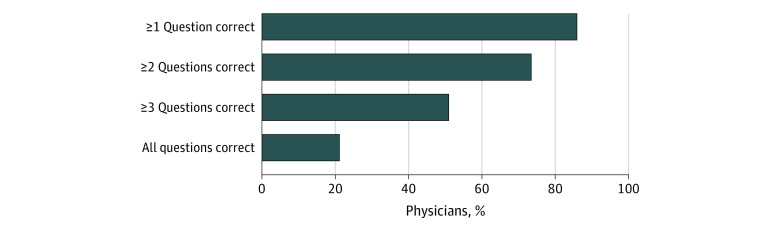
Results: The response rate was 45% (405 of 900) and 371 respondents met inclusion criteria. Among the respondents included in this study, 59% (n = 220) identified as male, 23% (n = 84) as Asian, 3% (n = 12) as Black, 6% (n = 24) as Hispanic, and 58% (n = 216) as White; 30% (n = 112) were primary care physicians, 35% (n = 128) were gastroenterologists, and 35% (n = 131) were rheumatologists; and the mean (SD) age was 49 (10) years. Overall, 52% of physicians (n = 192) accurately estimated costs before the deductible was met, 62% (n = 228) accurately used coinsurance information, 61% (n = 224) accurately used copay information, and 57% (n = 210) accurately estimated costs once the out-of-pocket maximum was met. Only 21% (n = 78) of physicians answered all 4 questions correctly. Ability to estimate out-of-pocket costs was not associated with specialty, attitudes toward cost conversations, or clinic characteristics.
Conclusions and relevance: This survey study found that many US physicians have difficulty estimating out-of-pocket costs, even when they have access to their patients' insurance plans. The mechanics involved in calculating real-time out-of-pocket costs are complex. These findings suggest that increased price transparency and simpler insurance cost-sharing mechanisms are needed to enable informed cost conversations at the point of prescribing.
Conflict of interest statement
Figures
References
-
- The Kaiser Family Foundation . Employer Health Benefits: 2020. Annual Survey. Published October 8, 2020. Accessed May 11, 2021. https://www.kff.org/health-costs/report/2020-employer-health-benefits-su...
-
- Collins SR, Rasmussen PW, Doty MM, Beutel S. The rise in health care coverage and affordability since health reform took effect: findings from the Commonwealth Fund Biennial Health Insurance Survey, 2014. Issue Brief (Commonw Fund). 2015;2:1-16. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
