

Assessment of Discrepancies Between Follow-up Infarct Volume and 90-Day Outcomes Among Patients With Ischemic Stroke Who Received Endovascular Therapy
- PMID: 34739060
- PMCID: PMC8571657
- DOI: 10.1001/jamanetworkopen.2021.32376
Assessment of Discrepancies Between Follow-up Infarct Volume and 90-Day Outcomes Among Patients With Ischemic Stroke Who Received Endovascular Therapy
Abstract
Importance: Some patients have poor outcomes despite small infarcts after endovascular therapy (EVT), while others with large infarcts do well. Understanding why these discrepancies occur may help to optimize EVT outcomes.
Objective: To validate exploratory findings from the Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE) trial regarding pretreatment, treatment-related, and posttreatment factors associated with discrepancies between follow-up infarct volume (FIV) and 90-day functional outcome.
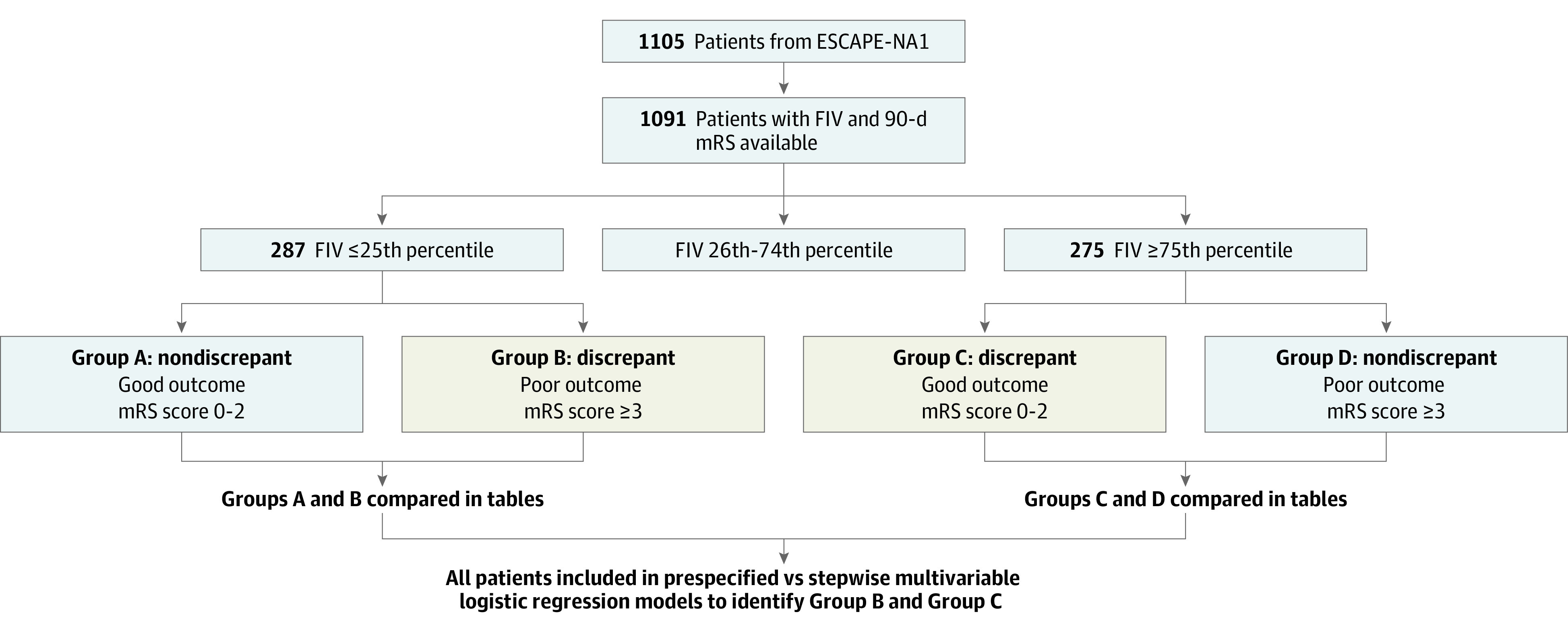
Design, setting, and participants: This cohort study is a post hoc analysis of the Safety and Efficacy of Nerinetide in Subjects Undergoing Endovascular Thrombectomy for Stroke (ESCAPE-NA1) trial, a double-blind, randomized, placebo-controlled, international, multicenter trial conducted from March 2017 to August 2019. Patients who participated in ESCAPE-NA1 and had available 90-day modified Rankin Scale (mRS) scores and 24-hour to 48-hour posttreatment follow-up parenchymal imaging were included.
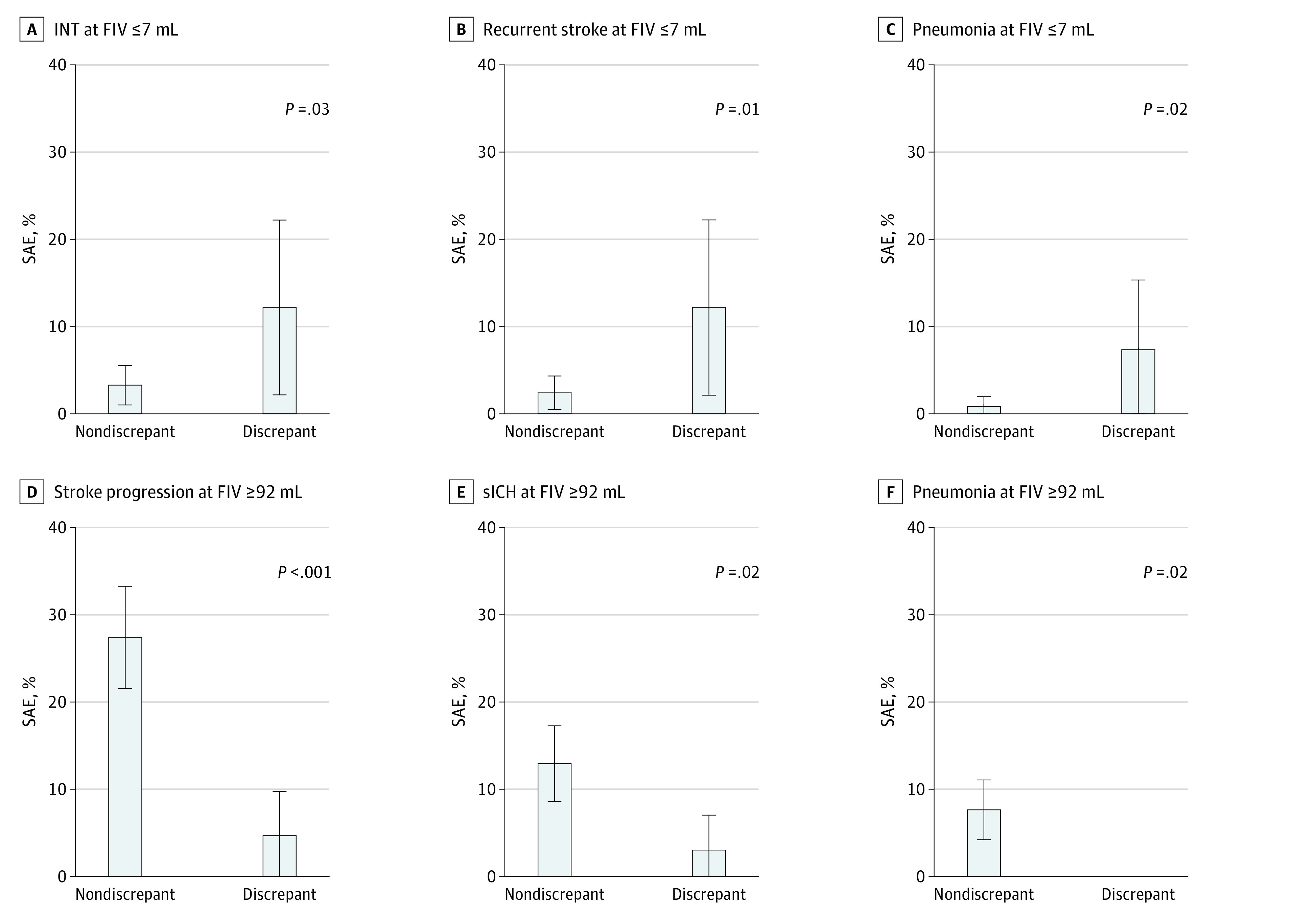
Exposures: Small FIV (volume ≤25th percentile) and large FIV (volume ≥75th percentile) on 24-hour computed tomography/magnetic resonance imaging. Baseline factors, outcomes, treatments, and poststroke serious adverse events (SAEs) were compared between discrepant cases (ie, patients with 90-day mRS score ≥3 despite small FIV or those with mRS scores ≤2 despite large FIV) and nondiscrepant cases.
Main outcomes and measures: Area under the curve (AUC) and goodness of fit of prespecified logistic models, including pretreatment (eg, age, cancer, vascular risk factors) and treatment-related and posttreatment (eg, SAEs) factors, were compared with stepwise regression-derived models for ability to identify small FIV with higher mRS score and large FIV with lower mRS score.
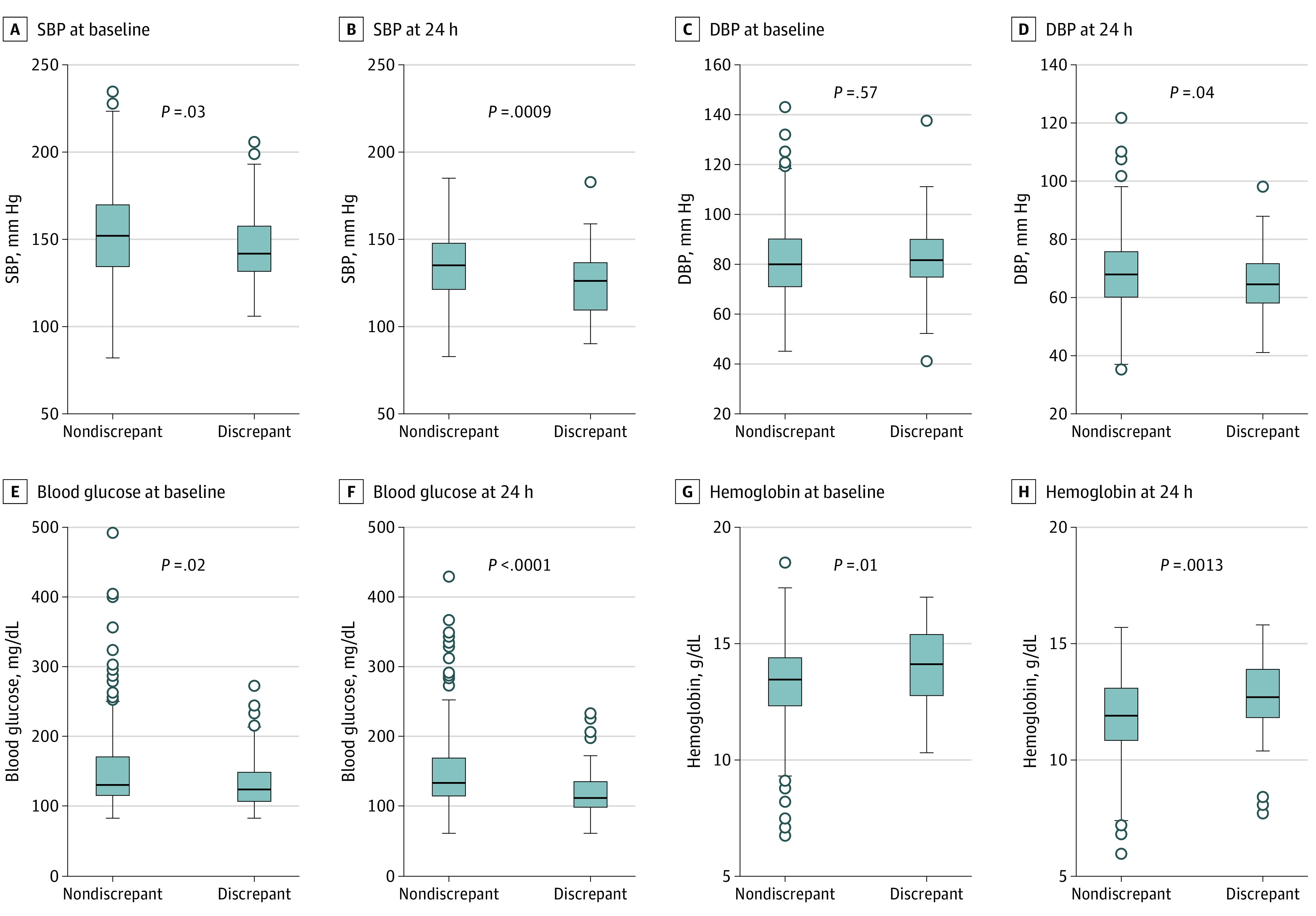
Results: Among 1091 patients (median [IQR] age, 70.8 [60.8-79.8] years; 549 [49.7%] women; median [IQR] FIV, 24.9 mL [6.6-92.2 mL]), 42 of 287 patients (14.6%) with FIV of 7 mL or less (ie, ≤25th percentile) had an mRS score of at least 3; 65 of 275 patients (23.6%) with FIV of 92 mL or greater (ie, ≥75th percentile) had an mRS score of 2 or less. Prespecified models of pretreatment factors (ie, age, cancer, vascular risk factors) associated with low FIV and higher mRS score performed similarly to models selected by stepwise regression (AUC, 0.92 [95% CI, 0.89-0.95] vs 0.93 [95% CI, 0.90-0.95]; P = .42). SAEs, specifically infarct in new territory, recurrent stroke, pneumonia, and congestive heart failure, were associated with low FIV and higher mRS scores; stepwise models also identified 24-hour hemoglobin as treatment-related/posttreatment factor (AUC, 0.92 [95% CI, 0.90-0.95] vs 0.94 [95% CI, 0.91-0.96]; P = .14). Younger age was associated with high FIV and lower mRS score; stepwise models identified absence of diabetes and higher baseline hemoglobin as additional pretreatment factors (AUC, 0.76 [95% CI, 0.70-0.82] vs 0.77 [95% CI, 0.71-0.83]; P = .82). Absence of SAEs, especially stroke progression, symptomatic intracerebral hemorrhage, and pneumonia, was associated with high FIV and lower mRS score2; stepwise models also identified 24-hour hemoglobin level, glucose, and diastolic blood pressure as posttreatment factors associated with discrepant cases (AUC, 0.80 [95% CI, 0.74-0.87] vs 0.79 [95% CI, 0.72-0.86]; P = .92).
Conclusions and relevance: In this study, discrepancies between functional outcome and post-EVT infarct volume were associated with differences in pretreatment factors, such as age and comorbidities, and posttreatment complications related to index stroke evolution, secondary prevention, and quality of stroke unit care. Besides preventing such complications, optimization of blood pressure, glucose levels, and hemoglobin levels are potentially modifiable factors meriting further study.
Conflict of interest statement
Figures
References
-
- Al-Ajlan FS, Al Sultan AS, Minhas P, et al. ; REVASCAT Investigators . Posttreatment infarct volumes when compared with 24-hour and 90-day clinical outcomes: insights from the REVASCAT randomized controlled trial. AJNR Am J Neuroradiol. 2018;39(1):107-110. doi:10.3174/ajnr.A5463 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
