

The Role of Palliative Care in COPD
- PMID: 34740592
- PMCID: PMC9131048
- DOI: 10.1016/j.chest.2021.10.032
The Role of Palliative Care in COPD
Abstract
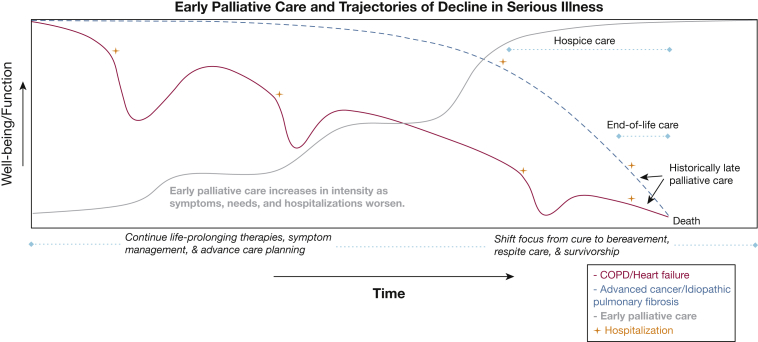
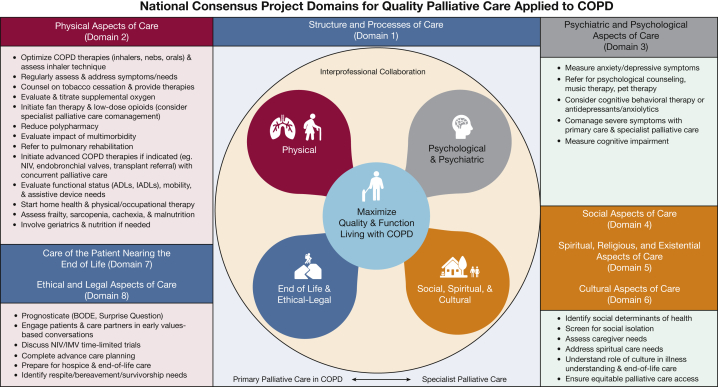
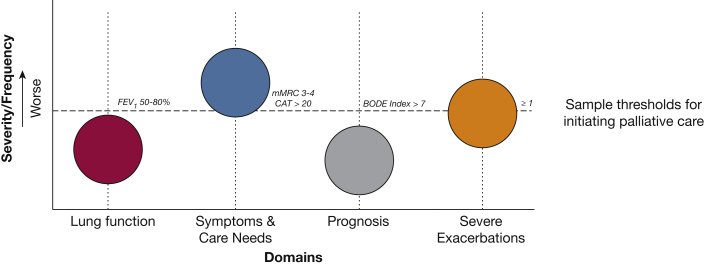
COPD is the fourth leading cause of death in the United States and is a serious respiratory illness characterized by years of progressively debilitating breathlessness, high prevalence of associated depression and anxiety, frequent hospitalizations, and diminished well-being. Despite the potential to confer significant quality-of-life benefits for patients and their care partners and to improve end-of-life (EOL) care, specialist palliative care is rarely implemented in COPD, and when initiated, it often occurs only at the very EOL. Primary palliative care delivered by frontline clinicians is a feasible model, but is not integrated routinely in COPD. In this review, we discuss the following: (1) the role of specialist and primary palliative care for patients with COPD and the case for earlier integration into routine practice; (2) the domains of the National Consensus Project Guidelines for Quality Palliative Care applied to people living with COPD and their care partners; and (3) triggers for initiating palliative care and practical ways to implement palliative care using case-based examples. This review solidifies that palliative care is much more than hospice and EOL care and demonstrates that early palliative care is appropriate at any point during the COPD trajectory. We emphasize that palliative care should be integrated long before the EOL to provide comprehensive support for patients and their care partners and to prepare them better for the EOL.
Keywords: COPD; end-of-life care; hospice care; palliative care.
Copyright © 2021 American College of Chest Physicians. All rights reserved.
Figures
References
-
- Han M.K., Martinez C.H., Au D.H., et al. Meeting the challenge of COPD care delivery in the USA: a multiprovider perspective. Lancet Respir Med. 2016;4(6):473–526. - PubMed
-
- Vogelmeier C.F., Criner G.J., Martinez F.J., et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 report: GOLD executive summary. Eur Respir J. 2017;195(5):557–582. - PubMed
-
- Strang S., Osmanovic M., Hallberg C., Strang P. Family caregivers’ heavy and overloaded burden in advanced chronic obstructive pulmonary disease. J Palliat Med. 2018;21(12):1768–1772. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
