

Increased complications of COVID-19 in people with cardiovascular disease: Role of the renin-angiotensin-aldosterone system (RAAS) dysregulation
- PMID: 34740598
- PMCID: PMC8563522
- DOI: 10.1016/j.cbi.2021.109738
Increased complications of COVID-19 in people with cardiovascular disease: Role of the renin-angiotensin-aldosterone system (RAAS) dysregulation
Abstract
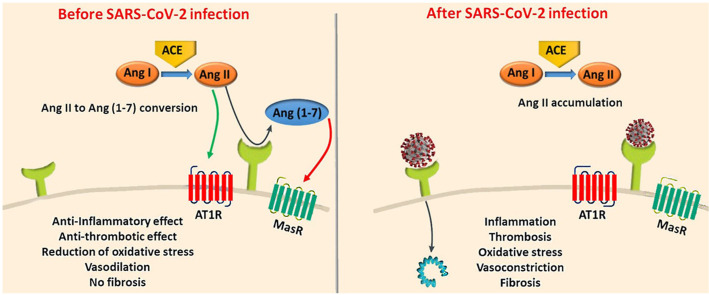
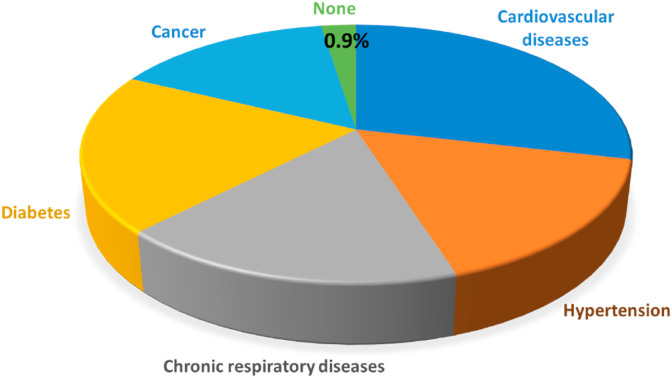
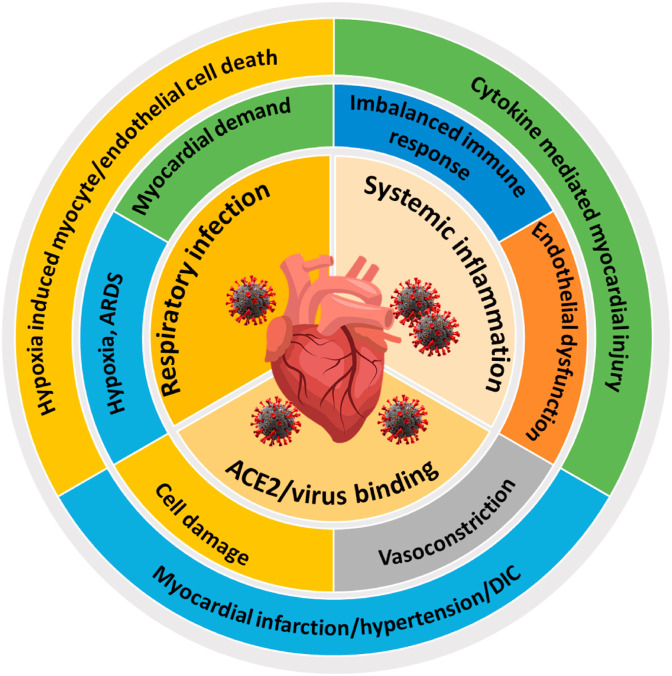
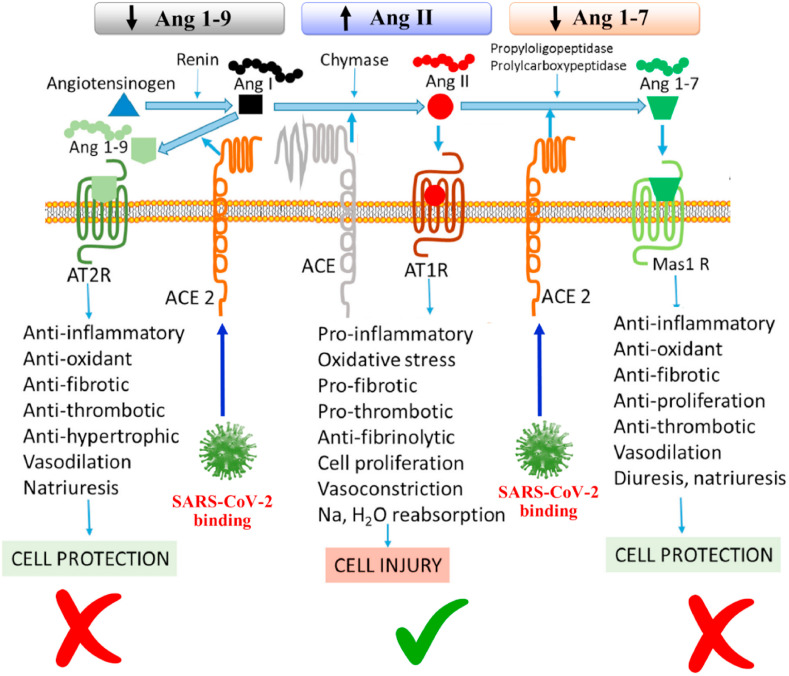
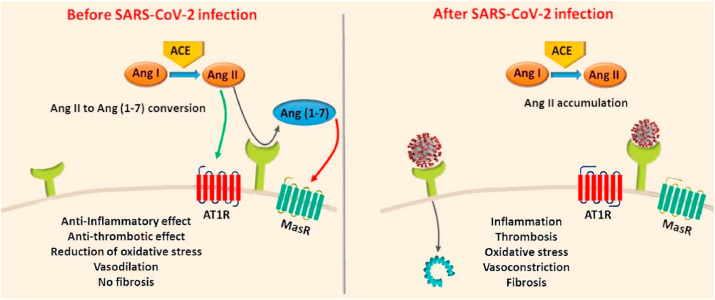
The rapid spread of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) that causes coronavirus disease 2019 (COVID-19), has had a dramatic negative impact on public health and economies worldwide. Recent studies on COVID-19 complications and mortality rates suggest that there is a higher prevalence in cardiovascular diseases (CVD) patients. Past investigations on the associations between pre-existing CVDs and susceptibility to coronavirus infections including SARS-CoV and the Middle East Respiratory Syndrome coronavirus (MERS-CoV), have demonstrated similar results. However, the underlying mechanisms are poorly understood. This has impeded adequate risk stratification and treatment strategies for CVD patients with SARS-CoV-2 infections. Generally, dysregulation of the expression of angiotensin-converting enzyme (ACE) and the counter regulator, angiotensin-converting enzyme 2 (ACE2) is a hallmark of cardiovascular risk and CVD. ACE2 is the main host receptor for SARS-CoV-2. Although further studies are required, dysfunction of ACE2 after virus binding and dysregulation of the renin-angiotensin-aldosterone system (RAAS) signaling may worsen the outcomes of people affected by COVID-19 and with preexisting CVD. Here, we review the current knowledge and outline the gaps related to the relationship between CVD and COVID-19 with a focus on the RAAS. Improved understanding of the mechanisms regulating viral entry and the role of RAAS may direct future research with the potential to improve the prevention and management of COVID-19.
Keywords: ACE2; COVID-19; Cardiovascular diseases; Coronavirus; RAAS; SARS-CoV-2.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
SARS-CoV-2 receptor ACE2-dependent implications on the cardiovascular system: From basic science to clinical implications.J Mol Cell Cardiol. 2020 Jul;144:47-53. doi: 10.1016/j.yjmcc.2020.04.031. Epub 2020 Apr 30. J Mol Cell Cardiol. 2020. PMID: 32360703 Free PMC article. Review.
-
Understanding the renin-angiotensin-aldosterone-SARS-CoV axis: a comprehensive review.Eur Respir J. 2020 Jul 9;56(1):2000912. doi: 10.1183/13993003.00912-2020. Print 2020 Jul. Eur Respir J. 2020. PMID: 32341103 Free PMC article. Review.
-
Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19).J Pathol. 2020 Jul;251(3):228-248. doi: 10.1002/path.5471. Epub 2020 Jun 10. J Pathol. 2020. PMID: 32418199 Free PMC article. Review.
-
Renin-Angiotensin-Aldosterone System (RAAS) Inhibitors and Coronavirus Disease 2019 (COVID-19).South Med J. 2021 Jan;114(1):51-56. doi: 10.14423/SMJ.0000000000001200. South Med J. 2021. PMID: 33398362 Free PMC article. Review.
-
What solid organ transplant healthcare providers should know about renin-angiotensin-aldosterone system inhibitors and COVID-19.Clin Transplant. 2020 Jul;34(7):e13991. doi: 10.1111/ctr.13991. Epub 2020 Jun 15. Clin Transplant. 2020. PMID: 32446267 Free PMC article. Review.
Cited by
-
COVID-19 and cardiovascular complications: updates of emergency medicine.Emerg Crit Care Med. 2023 Sep;3(3):104-114. doi: 10.1097/ec9.0000000000000095. Epub 2023 Jun 1. Emerg Crit Care Med. 2023. PMID: 38314258 Free PMC article.
-
Acute Cardiovascular Events After COVID-19 in England in 2020: A Self-Controlled Case Series Study.Clin Epidemiol. 2023 Sep 1;15:911-921. doi: 10.2147/CLEP.S421062. eCollection 2023. Clin Epidemiol. 2023. PMID: 37681195 Free PMC article.
-
Identification of potential biomarkers to predict organ morbidity in COVID-19: A repository based proteomics perspective.Biochem Biophys Rep. 2023 Sep;35:101493. doi: 10.1016/j.bbrep.2023.101493. Epub 2023 Jun 2. Biochem Biophys Rep. 2023. PMID: 37304132 Free PMC article.
-
Progranulin (PGRN) as a regulator of inflammation and a critical factor in the immunopathogenesis of cardiovascular diseases.J Inflamm (Lond). 2023 Jan 19;20(1):1. doi: 10.1186/s12950-023-00327-0. J Inflamm (Lond). 2023. PMID: 36658641 Free PMC article. Review.
-
Severe COVID-19 outcomes by cardiovascular risk profile in England in 2020: a population-based cohort study.Lancet Reg Health Eur. 2023 Apr;27:100604. doi: 10.1016/j.lanepe.2023.100604. Epub 2023 Mar 7. Lancet Reg Health Eur. 2023. PMID: 36911072 Free PMC article.
References
-
- Yoshikawa T., Hill T.E., Yoshikawa N., Popov V.L., Galindo C.L., Garner H.R., Peters C.J., Te Tseng C. Dynamic innate immune responses of human bronchial epithelial cells to severe acute respiratory syndrome-associated coronavirus infection. PLoS One. 2010;5 doi: 10.1371/journal.pone.0008729. - DOI - PMC - PubMed
-
- Gu J., Gong E., Zhang B., Zheng J., Gao Z., Zhong Y., Zou W., Zhan J., Wang S., Xie Z., Zhuang H., Wu B., Zhong H., Shao H., Fang W., Gao D., Pei F., Li X., He Z., Xu D., Shi X., Anderson V.M., Leong A.S.Y. Multiple organ infection and the pathogenesis of SARS. J. Exp. Med. 2005;202:415–424. doi: 10.1084/jem.20050828. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
