

Worldwide differences of hospitalization for ST-segment elevation myocardial infarction during COVID-19: A systematic review and meta-analysis
- PMID: 34740717
- PMCID: PMC8561779
- DOI: 10.1016/j.ijcard.2021.10.156
Worldwide differences of hospitalization for ST-segment elevation myocardial infarction during COVID-19: A systematic review and meta-analysis
Abstract
Background: Discrepant data were reported about hospital admissions for ST-segment elevation myocardial infarction (STEMI) during COVID-19 pandemic. We reviewed studies reporting STEMI hospitalizations during COVID-19 pandemic, investigating whether differences in COVID-19 epidemiology or public health-related factors could explain discrepant findings in different countries.
Methods: Search through MedLine, Embase, Scopus, Web-of-Science, Cochrane Register of Controlled Trials, of studies comparing STEMI admissions during COVID-19 pandemic with a reference period, without language restrictions, as registered in PROSPERO International Prospective Register of Systematic Reviews. Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines were followed. Data independently extracted by multiple investigators were pooled using a random-effects model. Health-related metrics were from publicly-available sources.
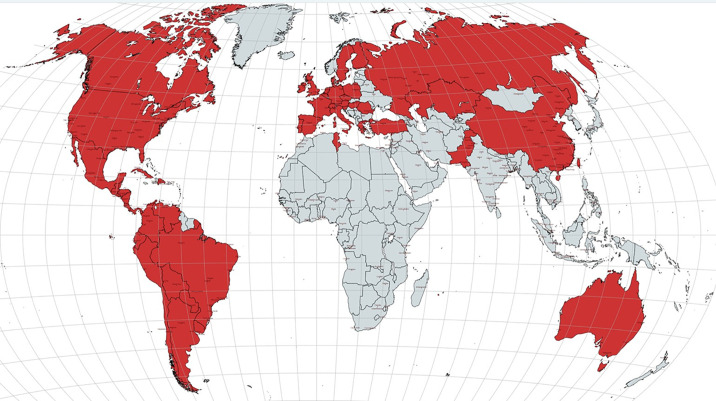
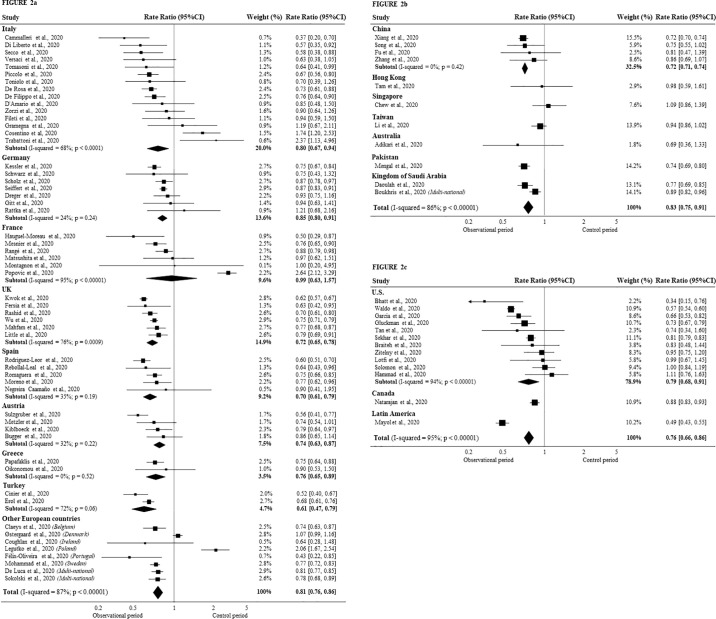
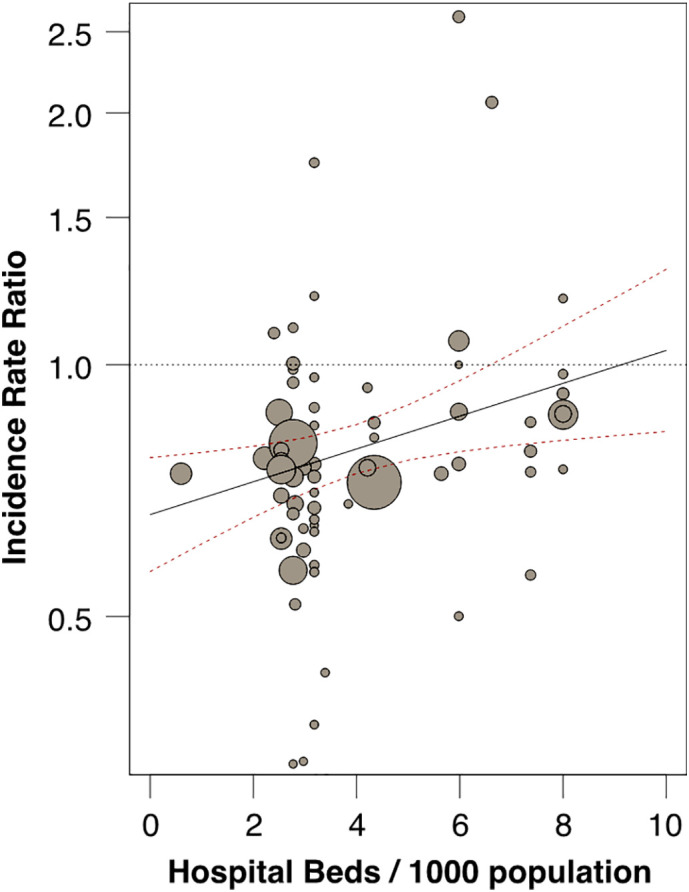
Results: We included 79 articles (111,557 STEMI cases, from 57 countries). During peak COVID-19 pandemic, overall incidence rate-ratio (IRR) of STEMI hospitalizations over reference period decreased (0.80; 95% CI 0.76-0.84; p < 0.05). Although wide variations and significant heterogeneity were detected among studies (I2 = 89%; p < 0.0001), no significant differences were observed by report methodology (survey vs registry), or observation/reference period. However, large differences emerged at country level not explained by COVID-related epidemiological data, nor by public health strategies. Instead, IRRs for STEMI admissions were inversely related to hospital bed availability in each country (p < 0.05).
Conclusions: During COVID-19 pandemic hospitalization for STEMI significantly decreased, although to a smaller extent than initially reported. Large variability emerged across countries, unrelated to COVID-related epidemiology or social containment measures. Disparities in healthcare organization likely contributed, indicating that proper organization of emergency medicine should be preserved during pandemics.
Keywords: Acute coronary syndromes; COVID-19; Healthcare organization; Myocardial infarction; STEMI; Sars-Cov-2.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
All authors declare: no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
Factors influencing medical care of STEMI patients during the COVID-19 pandemic worldwide.Int J Cardiol. 2022 Apr 1;352:195-196. doi: 10.1016/j.ijcard.2022.01.044. Epub 2022 Jan 23. Int J Cardiol. 2022. PMID: 35081423 Free PMC article. No abstract available.
References
-
- Kwong J.C., Schwartz K.L., Campitelli M.A., et al. Acute myocardial infarction after laboratory-confirmed influenza infection. N. Engl. J. Med. 2018;378(4):345–353. - PubMed
-
- Warren-Gash C., Blackburn R., Whitaker H., McMenamin J., Hayward A.C. Laboratory-confirmed respiratory infections as triggers for acute myocardial infarction and stroke: a self- controlled case series analysis of national linked datasets from Scotland. Eur. Respir. J. 2018;51(3):1701794. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
