

Evaluation of a contactless neonatal physiological monitor in Nairobi, Kenya
- PMID: 34740876
- PMCID: PMC9125375
- DOI: 10.1136/archdischild-2021-322344
Evaluation of a contactless neonatal physiological monitor in Nairobi, Kenya
Abstract
Background: Globally, 2.5 million neonates died in 2018, accounting for 46% of under-5 deaths. Multiparameter continuous physiological monitoring (MCPM) of neonates allows for early detection and treatment of life-threatening health problems. However, neonatal monitoring technology is largely unavailable in low-resource settings.
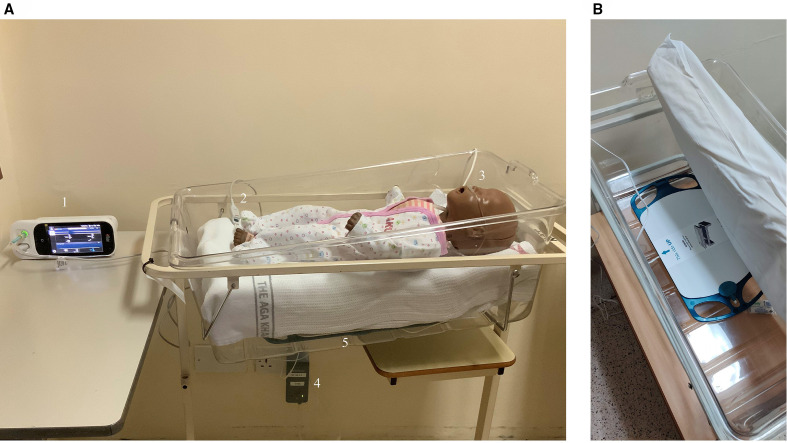
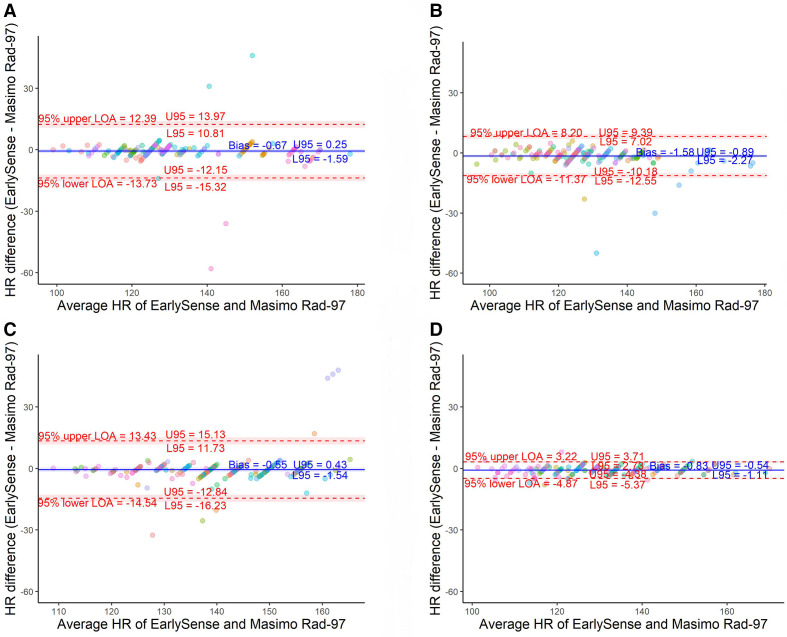
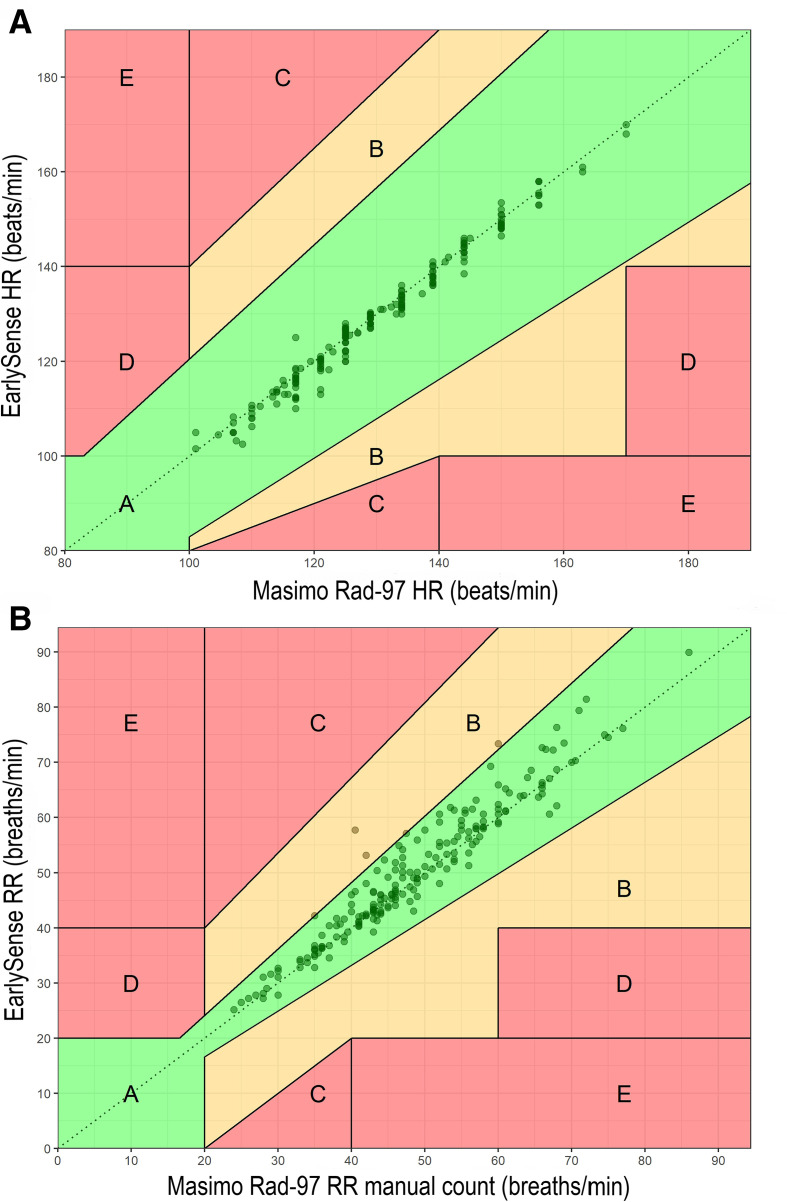
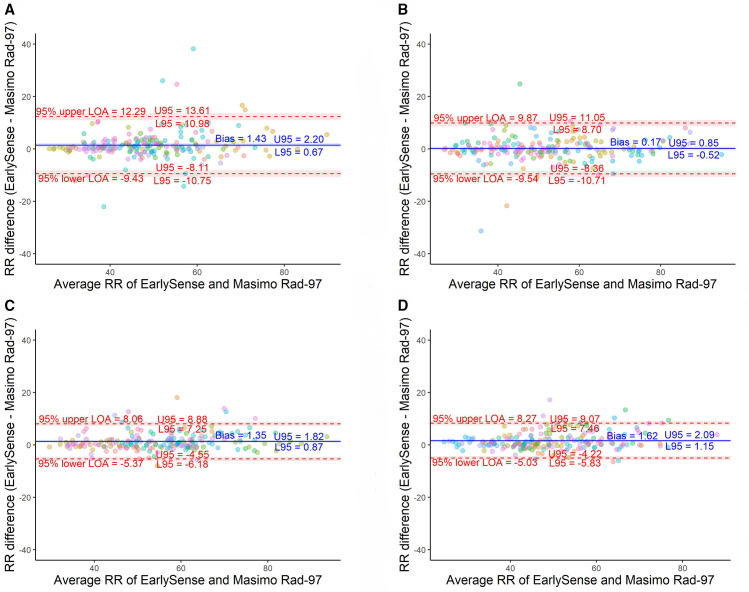
Methods: In four evaluation rounds, we prospectively compared the accuracy of the EarlySense under-mattress device to the Masimo Rad-97 pulse CO-oximeter with capnography reference device for heart rate (HR) and respiratory rate (RR) measurements in neonates in Kenya. EarlySense algorithm optimisations were made between evaluation rounds. In each evaluation round, we compared 200 randomly selected epochs of data using Bland-Altman plots and generated Clarke error grids with zones of 20% to aid in clinical interpretation.
Results: Between 9 July 2019 and 8 January 2020, we collected 280 hours of MCPM data from 76 enrolled neonates. At the final evaluation round, the EarlySense MCPM device demonstrated a bias of -0.8 beats/minute for HR and 1.6 breaths/minute for RR, and normalised spread between the 95% upper and lower limits of agreement of 6.2% for HR and 27.3% for RR. Agreement between the two MCPM devices met the a priori-defined threshold of 30%. The Clarke error grids showed that all observations for HR and 197/200 for RR were within a 20% difference.
Conclusion: Our research indicates that there is acceptable agreement between the EarlySense and Masimo MCPM devices in the context of large within-subject variability; however, further studies establishing cost-effectiveness and clinical effectiveness are needed before large-scale implementation of the EarlySense MCPM device in neonates.
Trial registration number: NCT03920761.
Keywords: intensive care units; neonatal; neonatology; technology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: YSH and RK are employed by EarlySense. All other authors declare no competing interests.
Figures
References
-
- World Health Organization . Newborns: improving survival and well-being, 2020. Available: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-morta... [Accessed 22 Jan 2021].
-
- United Nations . Ensure healthy lives and promote well-being for all at all ages, 2020. Available: https://sustainabledevelopment.un.org/sdg3; [Accessed 22 Jan 2021].
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous