

Neoadjuvant T-DM1/pertuzumab and paclitaxel/trastuzumab/pertuzumab for HER2+ breast cancer in the adaptively randomized I-SPY2 trial
- PMID: 34741023
- PMCID: PMC8571284
- DOI: 10.1038/s41467-021-26019-y
Neoadjuvant T-DM1/pertuzumab and paclitaxel/trastuzumab/pertuzumab for HER2+ breast cancer in the adaptively randomized I-SPY2 trial
Abstract
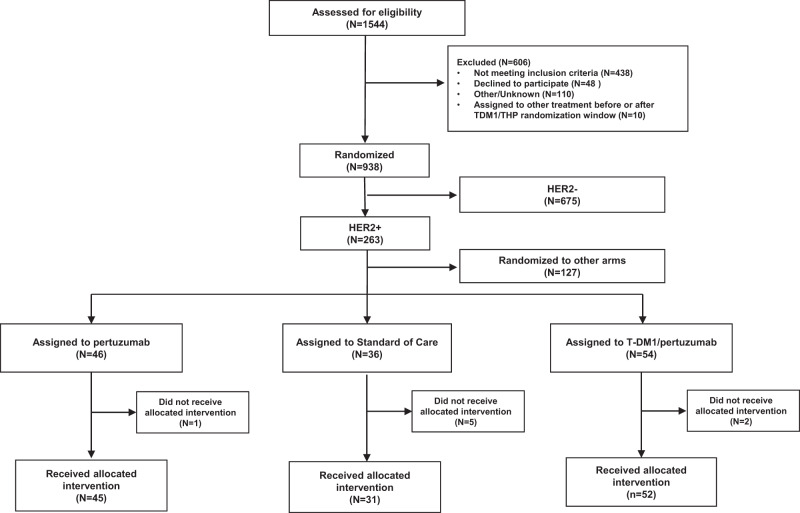
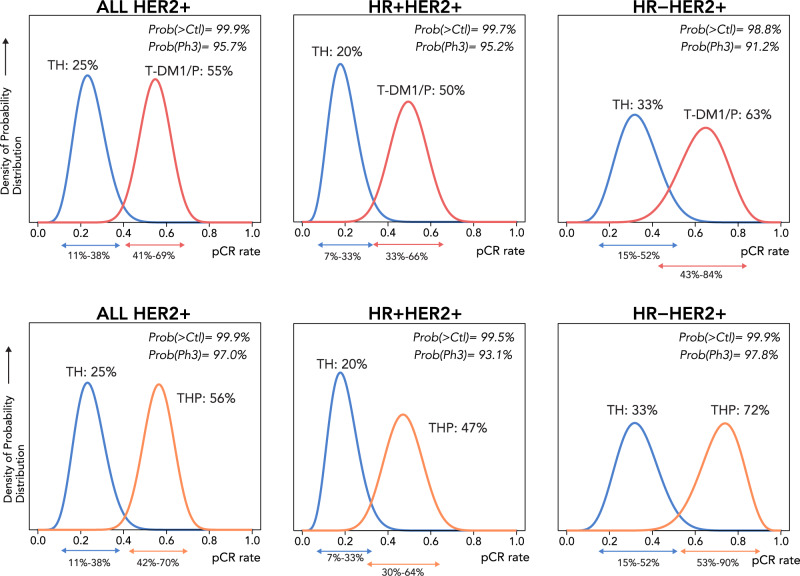
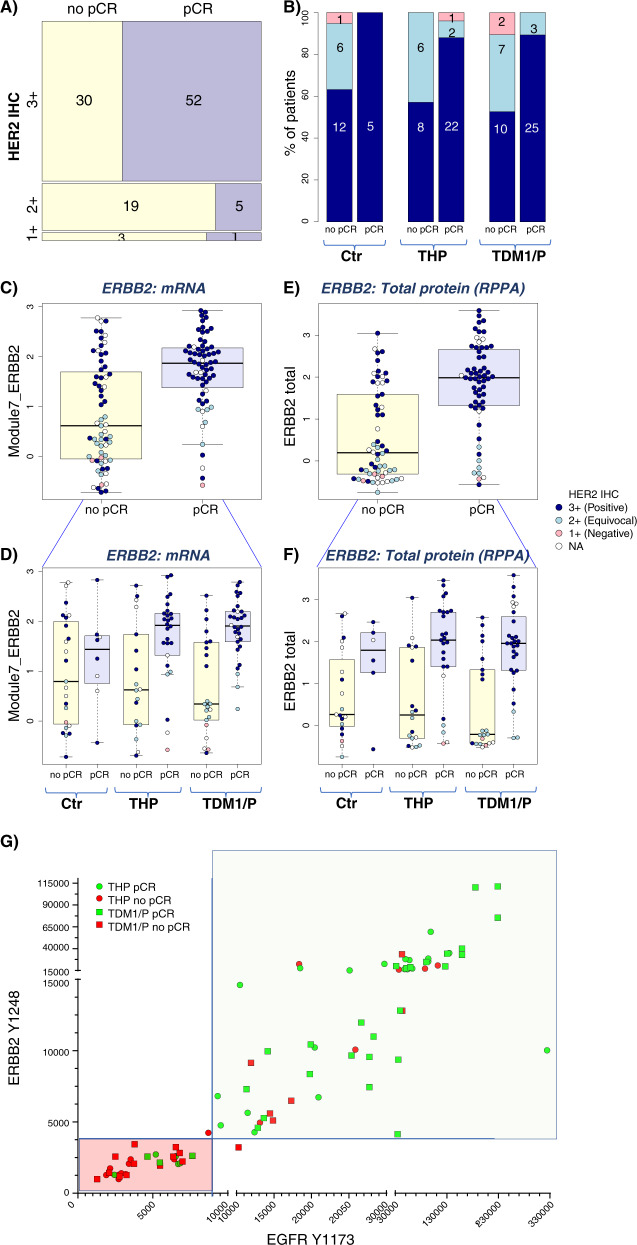
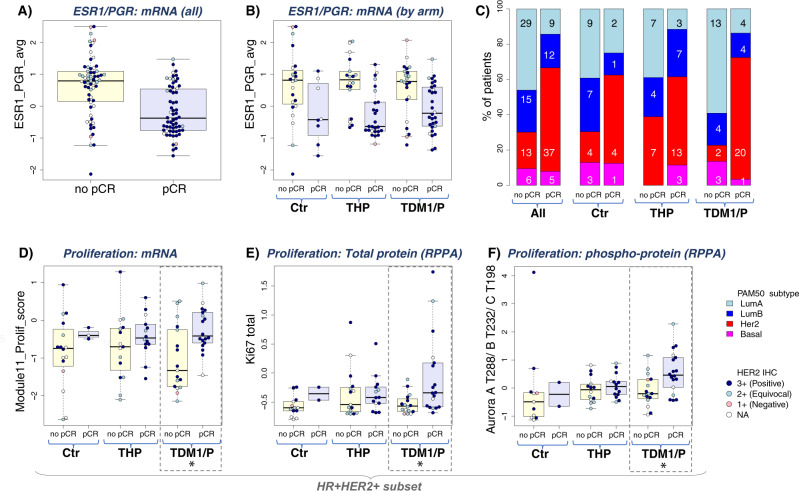
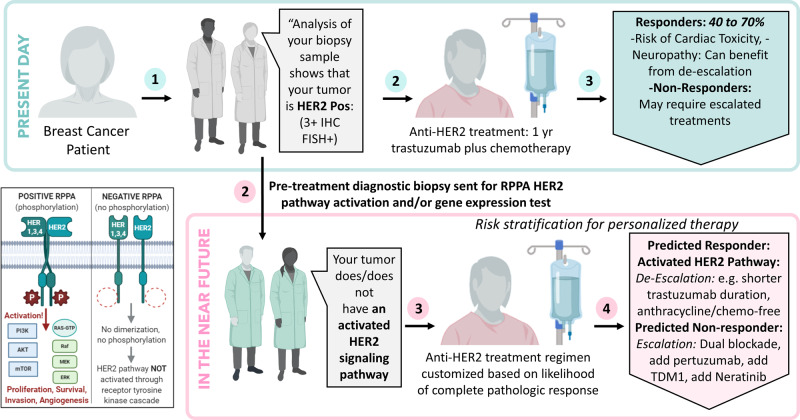
HER2-targeted therapy dramatically improves outcomes in early breast cancer. Here we report the results of two HER2-targeted combinations in the neoadjuvant I-SPY2 phase 2 adaptive platform trial for early breast cancer at high risk of recurrence: ado-trastuzumab emtansine plus pertuzumab (T-DM1/P) and paclitaxel, trastuzumab and pertuzumab (THP). Eligible women have >2.5 cm clinical stage II/III HER2+ breast cancer, adaptively randomized to T-DM1/P, THP, or a common control arm of paclitaxel/trastuzumab (TH), followed by doxorubicin/cyclophosphamide, then surgery. Both T-DM1/P and THP arms 'graduate' in all subtypes: predicted pCR rates are 63%, 72% and 33% for T-DM1/P (n = 52), THP (n = 45) and TH (n = 31) respectively. Toxicity burden is similar between arms. Degree of HER2 pathway signaling and phosphorylation in pretreatment biopsy specimens are associated with response to both T-DM1/P and THP and can further identify highly responsive HER2+ tumors to HER2-directed therapy. This may help identify patients who can safely de-escalate cytotoxic chemotherapy without compromising excellent outcome.
© 2021. The Author(s).
Conflict of interest statement
Amy S. Clark has received unrelated research support from Novartis. Christina Yau has consulted for NantOmics, LLC, part of the NantWorks network. E.F. Petricoin reports: leadership roles with: Perthera and Ceres Nanosciences; stock or other ownership interests in Perthera, Ceres Nanosciences and Avant Diagnostics; consulting or advisory roles with Perthera, Ceres Nanosciences, AZGen, Avant Diagnostics; institutional research support from Ceres Nanosciences, GlaxoSmithKline), Abbvie, Symphogen, and Genentech; patents, royalties, other intellectual property from National Institutes of Health patents licensing fee distribution/royalty, co-inventor on filed George Mason University–assigned patents related to phosphorylated HER2 and EGFR response predictors for HER family-directed therapeutics, as such can receive royalties and licensing distribution on any licensed IP; travel, accommodations, expenses received from Perthera and Ceres Nanosciences. Laura J. van ‘t Veer is a part-time employee and stockholder in Agendia N.V. Doug Yee has received unrelated research support from Boehringer Ingleheim. StacyMoulder has been an employee of Eli Lilly since 2021. A. Jo Chein reports institutional research support from Seagen, Merck, Amgen and Puma Biotechnology. Claudine Isaacs has received consulting fees from Seattle Genetics, Genentech, AstraZeneca, Novartis, PUMA, Pfizer, and Esai. Judy C. Boughey has received support from Eli Lilly. Barbara Haley reports that UTSouthwestern Medical Center Dallas receives funding for her research as PI from Pfizer, Lilly, Daiichi Sankyo, Roche, Puma, Astra Zeneca and Sanofi. Hyo S. Han reports institutional research support from GlaxoSmithKline, Abbvie, Prescient, G1 therapeutics, Marker therapeutics, Novartis, Horizon Pharma, Pfizer, Seattle Genetics, Arvinas and Zymeworks; she has received a grant from the Department of Defence and is a member of Lilly’ Speaker’s Bureau. Andres Forero-Torres became a Seattle Genetics employee in 2018 and holds stock option from this employment. Julie Lang has previously received a research grant from ANGLE Parsortix and has received honoraria as part of the Genomic Health’s speakers’ bureau and a Puma Biotechnology advisory board. Debu Tripathy receives research support from Novartis, Pfizer, Polyphor and has been a paid consultant for services on steering committees or advisory boards for Novartis, Pfizer, AstraZeneca, GlaxoSmithKline, OncoPep, Gilead, Exact Sciences. Rita Nanda has received research support from Arvinas, AstraZeneca, Celgene, Corcept Therapeutics, Genentech/Roche, Immunomedics/Gilead, Merck, OBI Pharm, Inc., Odonate Therapeutics, OncoSec, Pfizer, Taiho and SeaGen. J.D. Wulfkuhle received honoraria from DAVA Oncology and consults for Baylor College of Medicine. Melissa Paolini is an employee and stock holder in Arcus Biosciences. Donald Berry and Scott Berry are co-owners of Berry Consultants, LLC, a company that designs adaptive Bayesian clinical trials (including I-SPY 2) for pharmaceutical and medical device companies, NIH cooperative groups, patient advocacy groups, and international consortia. Hope Rugo reports institutional research support from Pfizer, Merck, Novartis, Lilly, Genentech, Odonate, Daiichi, Seattle Genetics, Eisai, Macrogenics, Sermonix, Boehringer Ingelheim, Polyphor, Astra Zeneca and Immunomedics, and has received honoraria from Puma Biotechnology, Mylan and Samsung. W. Fraser Symmans is a co-founder with equity in Delphi Diagnostics that licensed intellectual property, is a co-inventor of an issued patent for the algorithm to calculate residual cancer burden that is freely available on the internet, holds publicly traded shares in IONIS Pharmaceuticals and Eiger Biopharmaceuticals, and is an unpaid scientific advisor to Roche for translational research related to the KAITLIN trial and unpaid steering committee member for the KATHERINE trial. Laura Esserman is an unpaid member of the board of directors of Quantum Leap Healthcare Collaborative (QLHC) and received grant support from QLHC for the I-SPY2 Trial; she is a member of the Blue Cross/Blue Shield Medical Advisory Panel and receives reimbursement for her time and travel; Dr. Esserman has received unrelated research support from Merck. Angela DeMichele has received honoraria or consulting fees from Pfizer and Context Therapeutics and reports institutional research support from Novartis, Pfizer, Genentech, Calithera and Menarini. All other authors declare no competing interests.
Figures
References
-
- Carey LA, et al. Molecular heterogeneity and response to neoadjuvant human epidermal growth factor receptor 2 targeting in CALGB 40601, a randomized phase III trial of paclitaxel plus trastuzumab with or without lapatinib. J. Clin. Oncol. 2016;34:542–549. doi: 10.1200/JCO.2015.62.1268. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
