

Genome-wide analysis of 53,400 people with irritable bowel syndrome highlights shared genetic pathways with mood and anxiety disorders
- PMID: 34741163
- PMCID: PMC8571093
- DOI: 10.1038/s41588-021-00950-8
Genome-wide analysis of 53,400 people with irritable bowel syndrome highlights shared genetic pathways with mood and anxiety disorders
Abstract
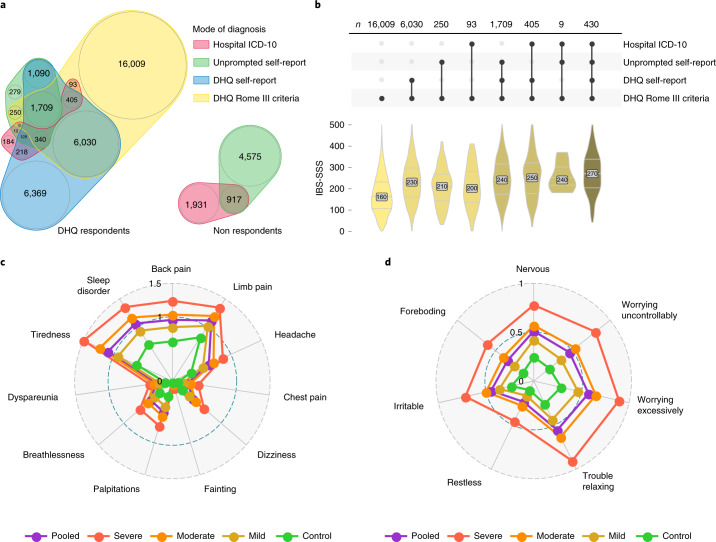
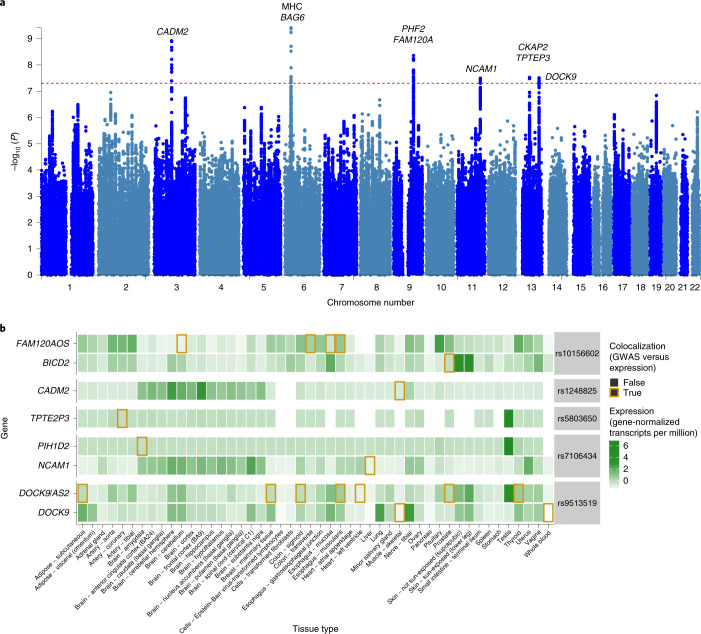
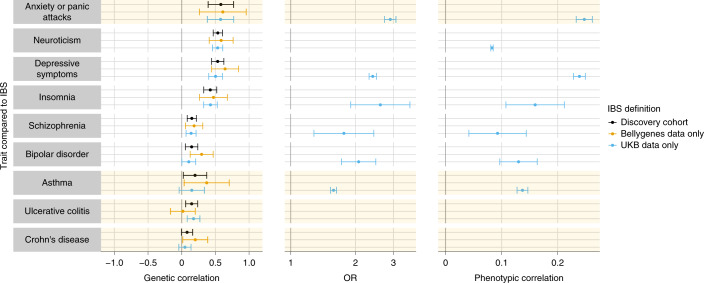
Irritable bowel syndrome (IBS) results from disordered brain-gut interactions. Identifying susceptibility genes could highlight the underlying pathophysiological mechanisms. We designed a digestive health questionnaire for UK Biobank and combined identified cases with IBS with independent cohorts. We conducted a genome-wide association study with 53,400 cases and 433,201 controls and replicated significant associations in a 23andMe panel (205,252 cases and 1,384,055 controls). Our study identified and confirmed six genetic susceptibility loci for IBS. Implicated genes included NCAM1, CADM2, PHF2/FAM120A, DOCK9, CKAP2/TPTE2P3 and BAG6. The first four are associated with mood and anxiety disorders, expressed in the nervous system, or both. Mirroring this, we also found strong genome-wide correlation between the risk of IBS and anxiety, neuroticism and depression (rg > 0.5). Additional analyses suggested this arises due to shared pathogenic pathways rather than, for example, anxiety causing abdominal symptoms. Implicated mechanisms require further exploration to help understand the altered brain-gut interactions underlying IBS.
© 2021. The Author(s).
Conflict of interest statement
C.A.A. and L.J. are paid consultants for Genomics. C.A.A. is a paid consultant for Celgene. J.S. and S.S. are employed by and hold stock or stock options in 23andMe. Members of the 23andMe research team are employed by and hold stock or stock options in 23andMe. P.J.W. has acted as a consultant or received research funding from Danone, Allergan, Ironwood Pharmaceuticals and Salix Pharmaceuticals, all outside of the submitted work. R.S. has accepted research grants from Sanofi and Zespri International and speaker fees from Alfawasserman. G.M. is a director of and shareholder in Genomics and partner in Peptide Groove LLP. The other authors declare no competing interests.
Figures
Comment in
-
Unravelling the genetics of irritable bowel syndrome.Nat Rev Gastroenterol Hepatol. 2022 Jan;19(1):5. doi: 10.1038/s41575-021-00556-9. Nat Rev Gastroenterol Hepatol. 2022. PMID: 34782784 No abstract available.
References
-
- Ford AC. Commentary: estimating the prevalence of IBS globally––past, present and future. Aliment. Pharmacol. Ther. 2020;51:198–199. - PubMed
-
- Gralnek IM, Hays RD, Kilbourne A, Naliboff B, Mayer EA. The impact of irritable bowel syndrome on health-related quality of life. Gastroenterology. 2000;119:654–660. - PubMed
-
- Hillilä MT, Färkkilä NJ, Färkkilä MA. Societal costs for irritable bowel syndrome—a population based study. Scand. J. Gastroenterol. 2010;45:582–591. - PubMed
-
- Longstreth GF, et al. Functional bowel disorders. Gastroenterology. 2006;130:1480–1491. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
