

Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): a cluster-randomised study
- PMID: 34741815
- PMCID: PMC8647163
- DOI: 10.1016/S0140-6736(21)01789-X
Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): a cluster-randomised study
Abstract
Background: Older adults with advanced cancer are at a high risk for treatment toxic effects. Geriatric assessment evaluates ageing-related domains and guides management. We examined whether a geriatric assessment intervention can reduce serious toxic effects in older patients with advanced cancer who are receiving high risk treatment (eg, chemotherapy).
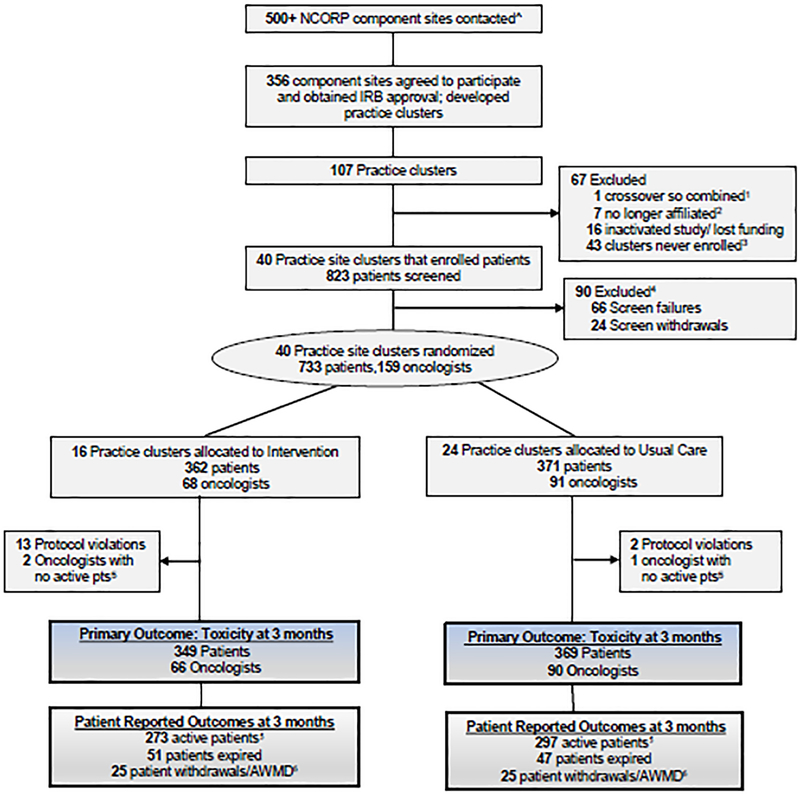
Methods: In this cluster-randomised trial, we enrolled patients aged 70 years and older with incurable solid tumours or lymphoma and at least one impaired geriatric assessment domain who were starting a new treatment regimen. 40 community oncology practice clusters across the USA were randomly assigned (1:1) to the intervention (oncologists received a tailored geriatric assessment summary and management recommendations) or usual care (no geriatric assessment summary or management recommendations were provided to oncologists) by means of a computer-generated randomisation table. The primary outcome was the proportion of patients who had any grade 3-5 toxic effect (based on National Cancer Institute Common Terminology Criteria for Adverse Events version 4) over 3 months. Practice staff prospectively captured toxic effects. Masked oncology clinicians reviewed medical records to verify. The study was registered with ClinicalTrials.gov, NCT02054741.
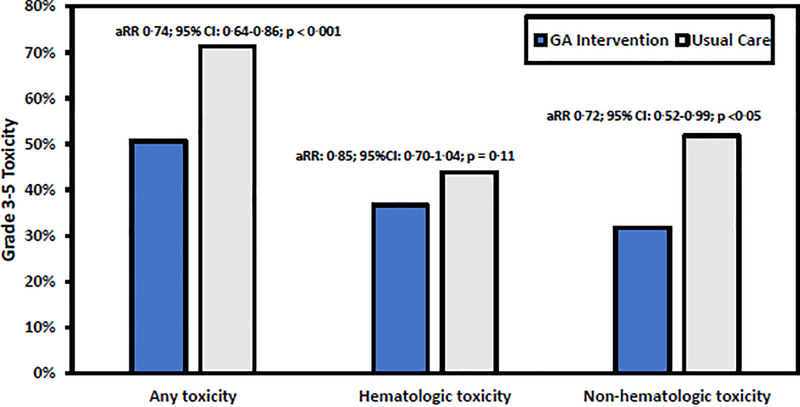
Findings: Between July 29, 2014, and March 13, 2019, we enrolled 718 patients. Patients had a mean age of 77·2 years (SD 5·4) and 311 (43%) of 718 participants were female. The mean number of geriatric assessment domain impairments was 4·5 (SD 1·6) and was not significantly different between the study groups. More patients in intervention group compared with the usual care group were Black versus other races (40 [11%] of 349 patients vs 12 [3%] of 369 patients; p<0·0001) and had previous chemotherapy (104 [30%] of 349 patients vs 81 [22%] of 369 patients; p=0·016). A lower proportion of patients in the intervention group had grade 3-5 toxic effects (177 [51%] of 349 patients) compared with the usual care group (263 [71%] of 369 patients; relative risk [RR] 0·74 (95% CI 0·64-0·86; p=0·0001). Patients in the intervention group had fewer falls over 3 months (35 [12%] of 298 patients vs 68 [21%] of 329 patients; adjusted RR 0·58, 95% CI 0·40-0·84; p=0·0035) and had more medications discontinued (mean adjusted difference 0·14, 95% CI 0·03-0·25; p=0·015).
Interpretation: A geriatric assessment intervention for older patients with advanced cancer reduced serious toxic effects from cancer treatment. Geriatric assessment with management should be integrated into the clinical care of older patients with advanced cancer and ageing-related conditions.
Funding: National Cancer Institute.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests KPL reports consultant fees from Pfizer and Seattle Genetics and honoraria from Pfizer. RFD received honoraria for consulting from Exelixis. TW reports research funding from Janssen and consultant fees from Seattle Genetics and Carevive. All other authors declare no competing interests.
Figures
Comment in
-
Geriatric assessment in older patients with cancer: a new standard of care.Lancet. 2021 Nov 20;398(10314):1853-1855. doi: 10.1016/S0140-6736(21)01998-X. Epub 2021 Nov 3. Lancet. 2021. PMID: 34741813 No abstract available.
-
[Geriatric assessment to improve geriatric oncology].Ned Tijdschr Geneeskd. 2022 Jan 24;166:D6572. Ned Tijdschr Geneeskd. 2022. PMID: 35138757 Dutch.
References
-
- Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002; 346(14): 1061–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
