

Estimation of DAPT Study Treatment Effects in Contemporary Clinical Practice: Findings From the EXTEND-DAPT Study
- PMID: 34743530
- PMCID: PMC8748407
- DOI: 10.1161/CIRCULATIONAHA.121.056878
Estimation of DAPT Study Treatment Effects in Contemporary Clinical Practice: Findings From the EXTEND-DAPT Study
Abstract
Background: Differences in patient characteristics, changes in treatment algorithms, and advances in medical technology could each influence the applicability of older randomized trial results to contemporary clinical practice. The DAPT Study (Dual Antiplatelet Therapy) found that longer-duration DAPT decreased ischemic events at the expense of greater bleeding, but subsequent evolution in stent technology and clinical practice may attenuate the benefit of prolonged DAPT in a contemporary population. We evaluated whether the DAPT Study population is different from a contemporary population of US patients receiving percutaneous coronary intervention and estimated the treatment effect of extended-duration antiplatelet therapy after percutaneous coronary intervention in this more contemporary cohort.
Methods: We compared the characteristics of drug-eluting stent-treated patients randomly assigned in the DAPT Study to a sample of more contemporary drug-eluting stent-treated patients in the National Cardiovascular Data Registry CathPCI Registry from July 2016 to June 2017. After linking trial and registry data, we used inverse-odds of trial participation weighting to account for patient and procedural characteristics and estimated a contemporary real-world treatment effect of 30 versus 12 months of DAPT after coronary stent procedures.
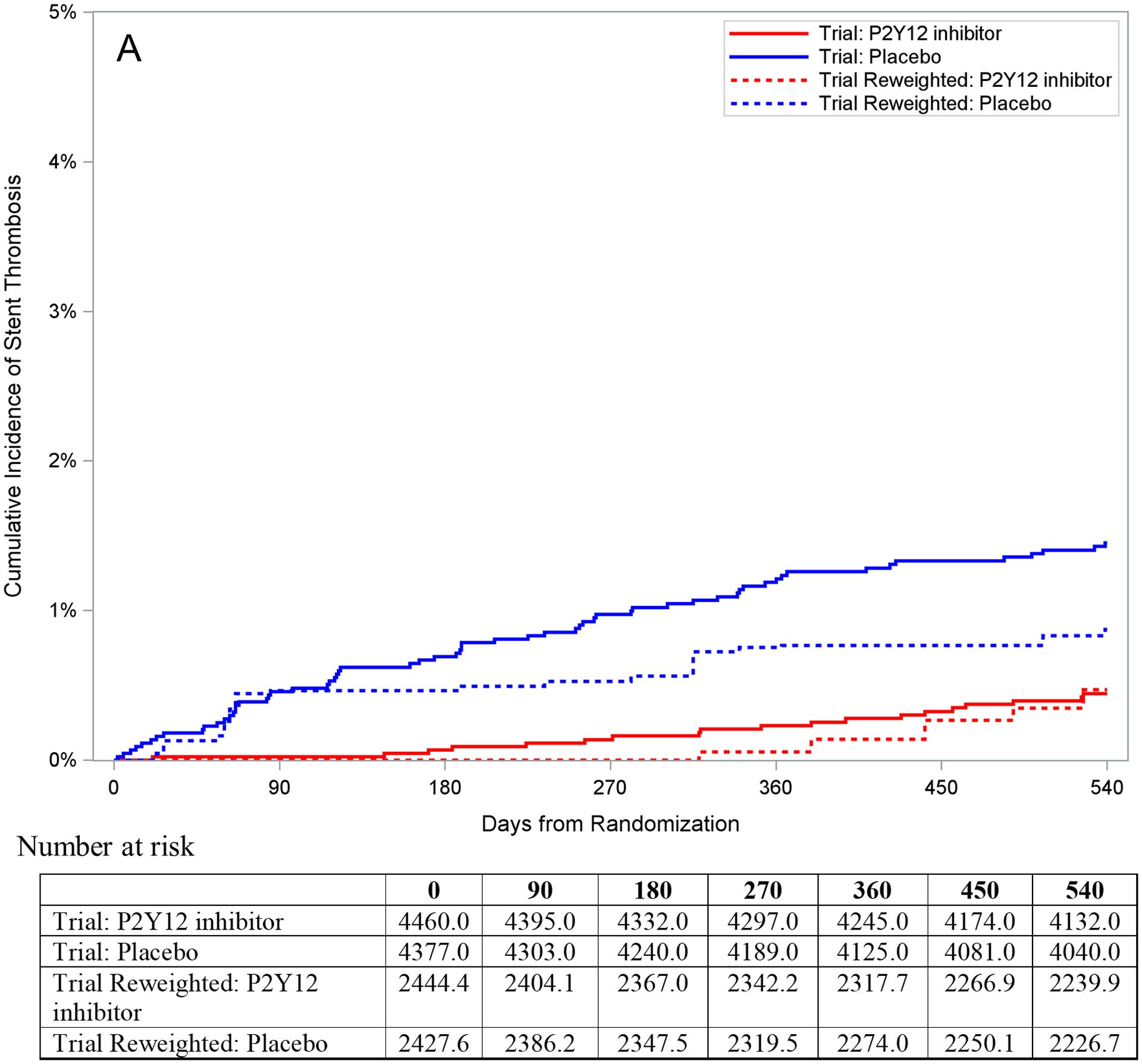
Results: The US drug-eluting stent-treated trial cohort included 8864 DAPT Study patients, and the registry cohort included 568 540 patients. Compared with the trial population, registry patients had more comorbidities and were more likely to present with myocardial infarction and receive 2nd-generation drug-eluting stents. After reweighting trial results to represent the registry population, there was no longer a significant effect of prolonged DAPT on reducing stent thrombosis (reweighted treatment effect: -0.40 [95% CI, -0.99% to 0.15%]), major adverse cardiac and cerebrovascular events (reweighted treatment effect, -0.52 [95% CI, -2.62% to 1.03%]), or myocardial infarction (reweighted treatment effect, -0.97% [95% CI, -2.75% to 0.18%]), but the increase in bleeding with prolonged DAPT persisted (reweighted treatment effect, 2.42% [95% CI, 0.79% to 3.91%]).
Conclusions: The differences between the patients and devices used in contemporary clinical practice compared with the DAPT Study were associated with the attenuation of benefits and greater harms attributable to prolonged DAPT duration. These findings limit the applicability of the average treatment effects from the DAPT Study in modern clinical practice.
Keywords: percutaneous coronary intervention; platelet aggregation inhibitors; pragmatic clinical trials as topic.
Figures




Comment in
-
The Evolution of Evidence-Based Medicine: When the Magic of the Randomized Clinical Trial Meets Real-World Data.Circulation. 2022 Jan 11;145(2):107-109. doi: 10.1161/CIRCULATIONAHA.121.057931. Epub 2022 Jan 10. Circulation. 2022. PMID: 35007161 No abstract available.
References
-
- Bonaca MP, Bhatt DL, Cohen M, Steg PG, Storey RF, Jensen EC, Magnani G, Bansilal S, Fish MP, Im K, et al. Long-Term Use of Ticagrelor in Patients with Prior Myocardial Infarction. New England Journal of Medicine. 2015;372:1791–1800. - PubMed
-
- Bittl JA, Baber U, Bradley SM and Wijeysundera DN. Duration of Dual Antiplatelet Therapy: A Systematic Review for the 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2016;68:1116–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
