

Granulomatous-Lymphocytic Interstitial Lung Disease Mimicking Sarcoidosis
- PMID: 34744421
- PMCID: PMC8552568
- DOI: 10.36141/svdld.v38i3.11114
Granulomatous-Lymphocytic Interstitial Lung Disease Mimicking Sarcoidosis
Abstract
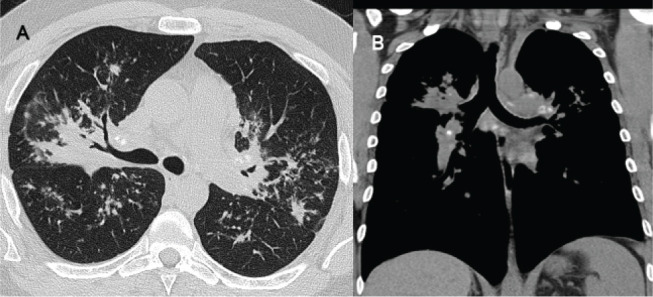
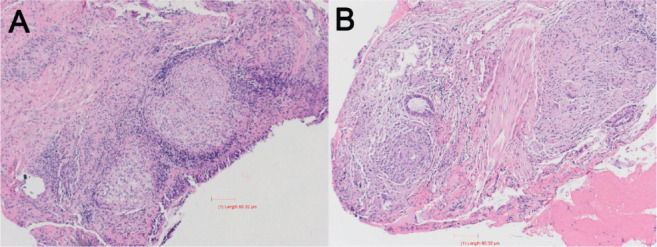
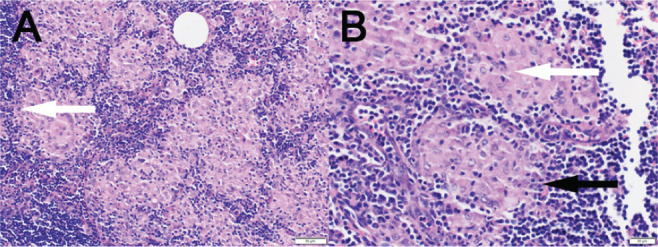
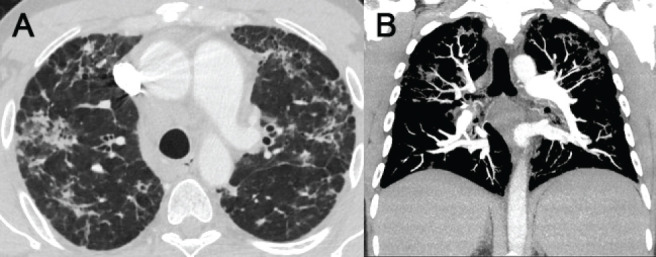
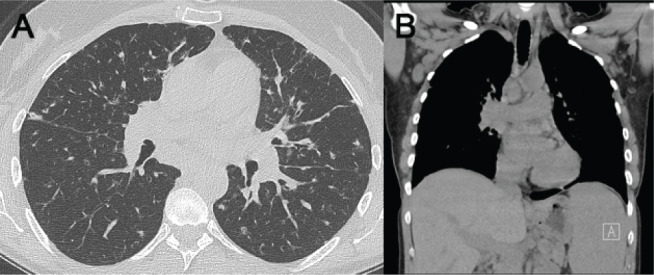
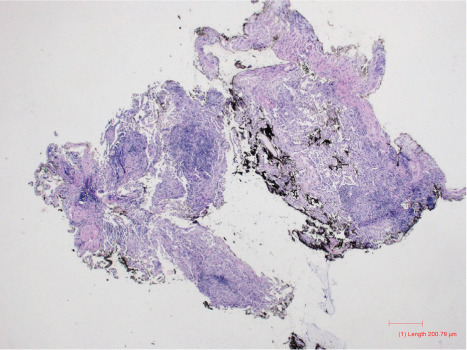
Common variable immunodeficiency (CVID) is one of the most common primary immunodeficiency disorders characterized by hypogammaglobulinemia and inadequate antibody response to immunizations. The impaired antibody response occurs due to the failure of B cells to differentiate into plasma cells resulting in low immunoglobulins levels and increased frequency of infections. Granulomatous and Lymphocytic Interstitial Lung Disease (GLILD) is a non-infectious complication of CVID that is seen in 10-30% of cases. GLILD is a multisystem inflammatory disease involving the lungs, lymph node, liver, spleen and gastrointestinal tract that mimics sarcoidosis. This report describes a series of cases who presented with dyspnea, recurrent respiratory infections or autoimmunity and on further evaluation revealed features suggestive of GLILD. There is very limited understanding of GLILD in terms of clinical presentation, the histo-pathological logical findings, and the diagnostic criteria by itself are limited. A diagnosis of GLILD is established in cases of CVID when there is evidence of lymphoproliferation, cytopenia, autoimmune processes and a lung biopsy demonstrating lymphocytic interstitial pneumonia, follicular bronchiolitis, lymphoid hyperplasia, and/or non-necrotizing granulomas. We review the treatment strategies, including replacement of immunoglobulin and agents targeting B and T lymphocytes. Systematic characterization of GLILD cases and long term follow up studies are sorely needed to understand the natural history of GLILD.
Keywords: CVID; Common variable immunodeficiency; GLILD; granulomatous lymphocytic interstitial lung disease; hypogammaglobulinemia.
Copyright: © 2021 SARCOIDOSIS VASCULITIS AND DIFFUSE LUNG DISEASES.
Figures
References
-
- Gathmann B, Mahlaoui N, Ceredih, et al. Clinical picture and treatment of 2212 patients with common variable immunodeficiency. J Allergy Clin Immunol. 2014;134(1):116–26. Epub 2014/03/04. doi: 10.1016/j.jaci.2013.12.1077. PubMed PMID: 24582312. - PubMed
-
- van de Ven AA, Compeer EB, van Montfrans JM, Boes M. B-cell defects in common variable immunodeficiency: BCR signaling, protein clustering and hardwired gene mutations. Crit Rev Immunol. 2011;31(2):85–98. Epub 2011/05/06. doi: 10.1615/critrevimmunol.v31.i2.10. PubMed PMID: 21542788. - PubMed
-
- Chun JK, Lee TJ, Song JW, Linton JA, Kim DS. Analysis of clinical presentations of Bruton disease: a review of 20 years of accumulated data from pediatric patients at Severance Hospital. Yonsei Med J. 2008;49(1):28–36. Epub 2008/02/29. doi: 10.3349/ymj.2008.49.1.28. PubMed PMID: 18306466; PubMed Central PMCID: PMCPMC2615253. - PMC - PubMed
-
- Maglione PJ. Autoimmune and Lymphoproliferative Complications of Common Variable Immunodeficiency. Curr Allergy Asthma Rep. 2016;16(3):19. Epub 2016/02/10. doi: 10.1007/s11882-016-0597-6. PubMed PMID: 26857017. - PubMed
LinkOut - more resources
Full Text Sources