

Pretreatment of Sulfonylureas Reducing Perihematomal Edema in Diabetic Patients With Basal Ganglia Hemorrhage: A Retrospective Case-Control Study
- PMID: 34744976
- PMCID: PMC8569795
- DOI: 10.3389/fneur.2021.736383
Pretreatment of Sulfonylureas Reducing Perihematomal Edema in Diabetic Patients With Basal Ganglia Hemorrhage: A Retrospective Case-Control Study
Abstract
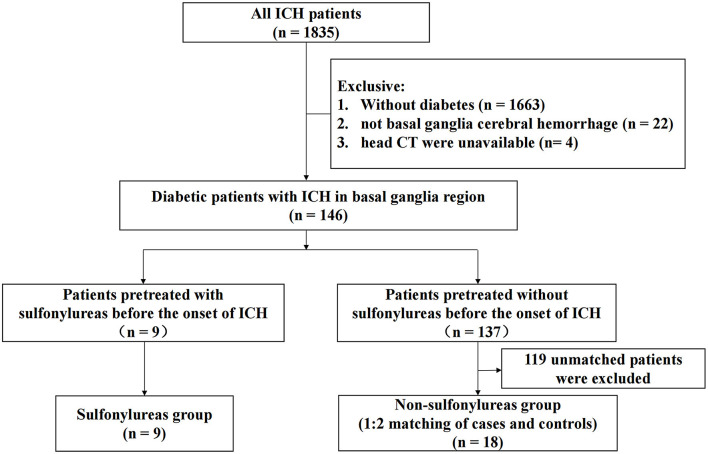
Background: The sulfonylurea receptor 1-transient receptor potential melastatin 4 (SUR1-TRPM4) channel is a target key mediator of brain edema. Sulfonylureas (SFUs) are blockers of the SUR1-TRPM4 channel. We made two assessments for the pretreatment of SFUs: (1) whether it associates with lower perihematomal edema (PHE) and (2) whether it associates with improved clinical outcomes in diabetic patients who have acute basal ganglia hemorrhage. Methods: This retrospective case-control study was conducted in diabetic adults receiving regular SFUs before the onset of intracerebral hemorrhage (ICH). All of the patients received the clinical diagnosis of spontaneous basal ganglia hemorrhage. The diagnosis was confirmed by a CT scan within 7 days after hemorrhage. For each case, we selected two matched controls with basal ganglia hemorrhage based on admission time (≤5 years) and age differences (≤5 years), with the same gender and similar hematoma volume. The primary outcome was PHE volume, and the secondary outcomes were relative PHE (rPHE), functional independence according to modified Rankin Scale score and Barthel Index at discharge, and death rate in the hospital. Results: A total of 27 patients (nine cases and 18 matched controls), admitted between January 1, 2009 and October 31, 2018, were included in our study. There was no significant association between SFU patients and non-SFU patients on PHE volumes [15.4 (7.4-50.2 ml) vs. 8.0 (3.1-22.1) ml, p = 0.100]. Compared to non-SFU patients, the SFU patients had significantly lower rPHE [0.8 (0.7-1.3) vs. 1.5 (1.2-1.9), p = 0.006]. After we adjusted the confounding factors, we found that sulfonylureas can significantly reduce both PHE volume (regression coefficient: -13.607, 95% CI: -26.185 to -1.029, p = 0.035) and rPHE (regression coefficient: -0.566, 95% CI: -0.971 to -0.161, p = 0.009). However, we found no significant improvement in clinical outcomes at discharge, in the event of pretreatment of SFUs before the onset of ICH, even after we adjusted the confounding factors. Conclusion: For diabetic patients with acute basal ganglia hemorrhage, pretreatment of sulfonylureas may associate with lower PHE and relative PHE on admission. No significant effect was found on the clinical outcomes when the patients were discharged. Future studies are needed to assess the potential clinical benefits using sulfonylureas for ICH patients.
Keywords: case-control study; intracerebral hemorrhage; perihematomal edema; prognosis; sulfonylureas.
Copyright © 2021 Jingjing, Jingjing, Bo, Le, Jingya, Dong, Fang and Wen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Sheth KN, Elm JJ, Molyneaux BJ, Hinson H, Beslow LA, Sze GK, et al. . Safety and efficacy of intravenous glyburide on brain swelling after large hemispheric infarction (GAMES-RP): a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. (2016) 15:1160–9. 10.1016/S1474-4422(16)30196-X - DOI - PubMed
LinkOut - more resources
Full Text Sources