

Anatomical Variations and Relationships of the Infratemporal Fossa: Foundation of a Novel Endonasal Approach to the Foramen Ovale
- PMID: 34745835
- PMCID: PMC8563275
- DOI: 10.1055/s-0040-1715815
Anatomical Variations and Relationships of the Infratemporal Fossa: Foundation of a Novel Endonasal Approach to the Foramen Ovale
Abstract
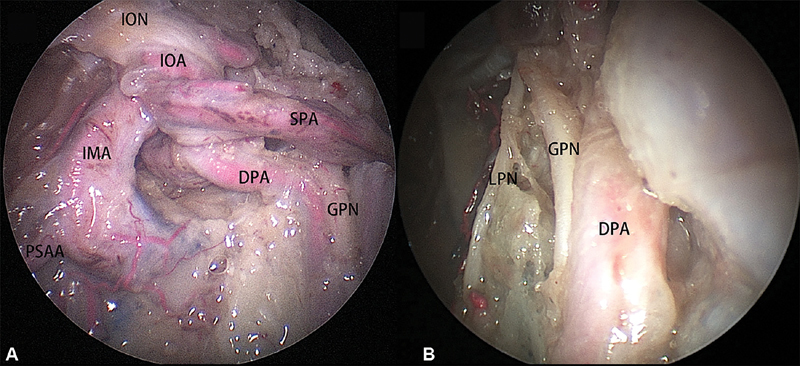
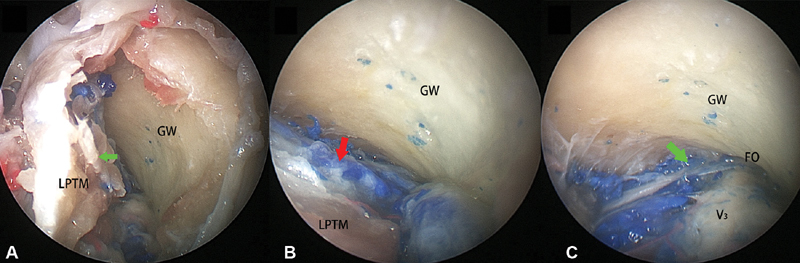
Objective Access to the infratemporal fossa (ITF) is complicated by its complex neurovascular relationships. In addition, copious bleeding from the pterygoid plexus adds to surgical challenge. This study aims to detail the anatomical relationships among the internal maxillary artery (IMA), pterygoid plexus, V 3, and pterygoid muscles in ITF. Furthermore, it introduces a novel approach that displaces the lateral pterygoid plate (LPP) to access the foramen ovale. Design and Main Outcome Measures Six cadaveric specimens (12 sides) were dissected using an endonasal approach to the ITF modified by releasing and displacing the LPP and lateral pterygoid muscle (LPTM) as a unit. Subperiosteal elevation of the superior head of LPTM revealed the foramen ovale. The anatomic relationships among the V 3 , pterygoid muscles, pterygoid plexus, and IMA were surveyed. Results In 9/12 sides (75%), the proximal IMA ran between the temporalis and the LPTM, whereas in 3/12 sides (25%), the IMA pierced the LPTM. The deep temporal nerve was a consistent landmark to separate the superior and inferior heads of LPTM. An endonasal approach displacing the LPP in combination with a subperiosteal elevation of the superior head of LPTM provided access to the posterior trunk of V 3 and foramen ovale while sparing injury of the LPTM and exposing the pterygoid plexus. The anterior trunk of V 3 traveled anterolaterally along the greater wing of sphenoid in all specimens. Conclusion Displacement of the LPP and LPTM provided direct exposure of foramen ovale and V 3 avoiding dissection of the muscle and pterygoid plexus; thus, this maneuver may prevent intraoperative bleeding and postoperative trismus.
Keywords: V 3; foramen ovale; infratemporal fossa; internal maxillary artery; lateral pterygoid plate.
Thieme. All rights reserved.
Conflict of interest statement
Conflict of Interest N.R.L. holds stock in Navigen Pharmaceuticals and was a consultant for Cooltech Inc. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures






References
-
- Kassam A, Snyderman C H, Mintz A, Gardner P, Carrau R L. Expanded endonasal approach: the rostrocaudal axis. Part I. Crista galli to the sella turcica. Neurosurg Focus. 2005;19(01):E3. - PubMed
-
- Kassam A, Snyderman C H, Mintz A, Gardner P, Carrau R L. Expanded endonasal approach: the rostrocaudal axis. Part II. posterior clinoids to the foramen magnum. Neurosurg Focus. 2005;19(01):E4. - PubMed
-
- Prevedello D M, Doglietto F, Jane J A, Jr, Jagannathan J, Han J, Laws E R., Jr History of endoscopic skull base surgery: its evolution and current reality. J Neurosurg. 2007;107(01):206–213. - PubMed
-
- Kassam A B, Snyderman C, Gardner P, Carrau R, Spiro R.The expanded endonasal approach: a fully endoscopic transnasal approach and resection of the odontoid process: technical case report Neurosurgery 20055701E213, discussion E213 - PubMed
-
- Gardner P A, Kassam A B, Thomas A.Endoscopic endonasal resection of anterior cranial base meningiomas Neurosurgery 2008630136–52., discussion 52–54 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
