

Predicting the Initial Treatment Response to Transarterial Chemoembolization in Intermediate-Stage Hepatocellular Carcinoma by the Integration of Radiomics and Deep Learning
- PMID: 34745952
- PMCID: PMC8566880
- DOI: 10.3389/fonc.2021.730282
Predicting the Initial Treatment Response to Transarterial Chemoembolization in Intermediate-Stage Hepatocellular Carcinoma by the Integration of Radiomics and Deep Learning
Abstract
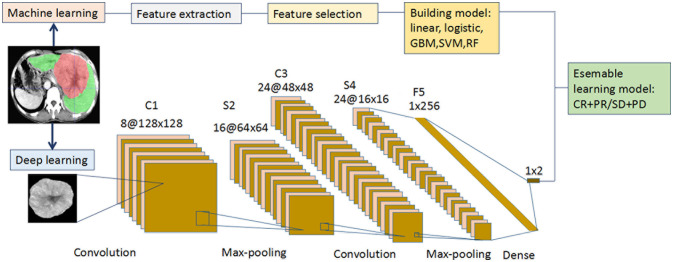
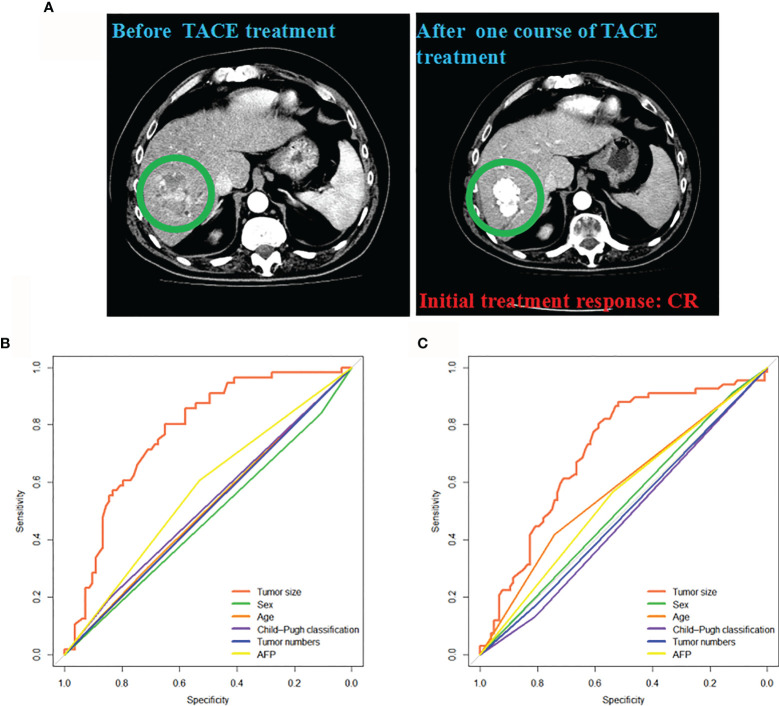
Objectives: We aimed to develop radiology-based models for the preoperative prediction of the initial treatment response to transarterial chemoembolization (TACE) in patients with hepatocellular carcinoma (HCC) since the integration of radiomics and deep learning (DL) has not been reported for TACE.
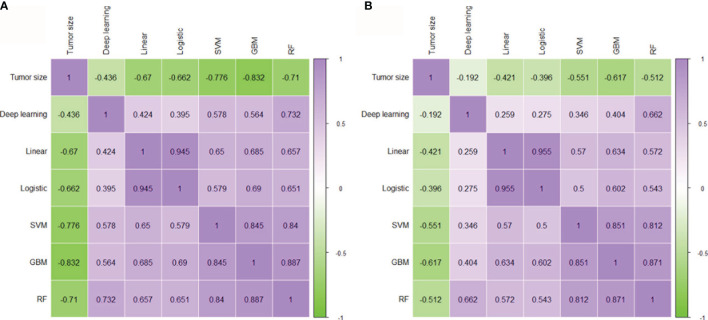
Methods: Three hundred and ten intermediate-stage HCC patients who underwent TACE were recruited from three independent medical centers. Based on computed tomography (CT) images, recursive feature elimination (RFE) was used to select the most useful radiomics features. Five radiomics conventional machine learning (cML) models and a DL model were used for training and validation. Mutual correlations between each model were analyzed. The accuracies of integrating clinical variables, cML, and DL models were then evaluated.
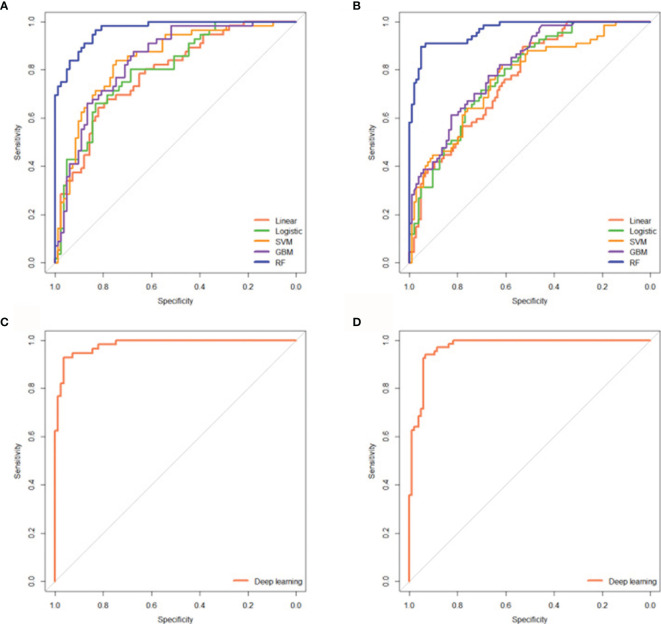
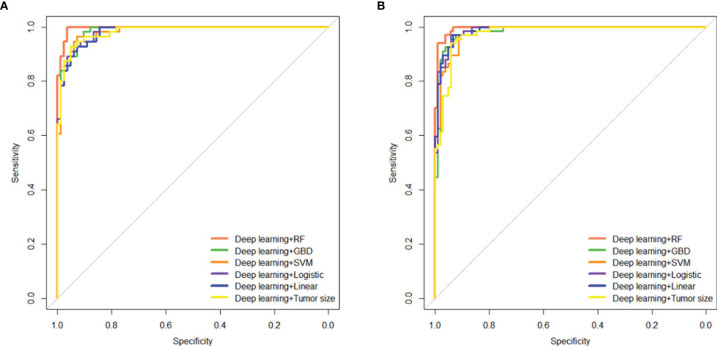
Results: Good predictive accuracies were showed across the two cohorts in the five cML models, especially the random forest algorithm (AUC = 0.967 and 0.964, respectively). DL showed high accuracies in the training and validation cohorts (AUC = 0.981 and 0.972, respectively). Significant mutual correlations were revealed between tumor size and the five cML models and DL model (each P < 0.001). The highest accuracies were achieved by integrating DL and the random forest algorithm in the training and validation cohorts (AUC = 0.995 and 0.994, respectively).
Conclusion: The radiomics cML models and DL model showed notable accuracy for predicting the initial response to TACE treatment. Moreover, the integrated model could serve as a novel and accurate method for prediction in intermediate-stage HCC.
Keywords: TACE; deep learning; hepatocellular carcinoma; machine learning; treatment response.
Copyright © 2021 Peng, Huang, Huang and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Zhuang BW, Li W, Wang W, Li B, Lu MD, Kuang M, et al. . Treatment Effect of Radiofrequency Ablation Versus Liver Transplantation and Surgical Resection for Hepatocellular Carcinoma Within Milan Criteria: A Population-Based Study. Eur Radiol (2021) 31(7):5379–89. doi: 10.1007/s00330-020-07551-9 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous