

Small conductance calcium activated K+ channel inhibitor decreases stretch induced vulnerability to atrial fibrillation
- PMID: 34746364
- PMCID: PMC8554272
- DOI: 10.1016/j.ijcha.2021.100898
Small conductance calcium activated K+ channel inhibitor decreases stretch induced vulnerability to atrial fibrillation
Abstract
Background: Atrial dilation is an important risk factor for atrial fibrillation (AF) and animal studies have found that acute atrial dilation shortens the atrial effective refractory period (AERP) and increases the risk of AF. Stretch activated ion channels (SACs) and calcium channels play a role in this. The expression profile and calcium dependent activation makes the small conductance calcium activated K+ channel (KCa2.x) a candidate for coupling stretch induced increases in intracellular calcium through K+-efflux and thereby shortening of atrial refractoriness.
Objectives: We hypothesized that KCa2.x channel inhibitors can prevent the stretch induced shortening of AERP and protect the heart from AF.
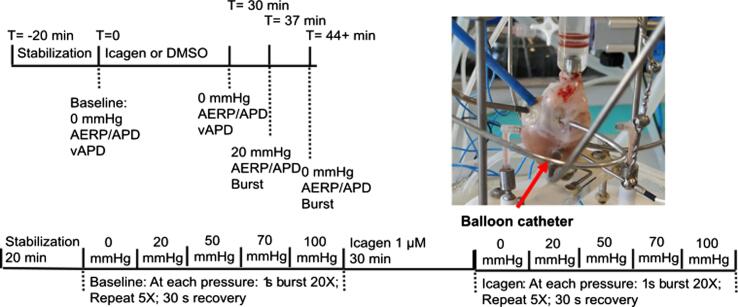
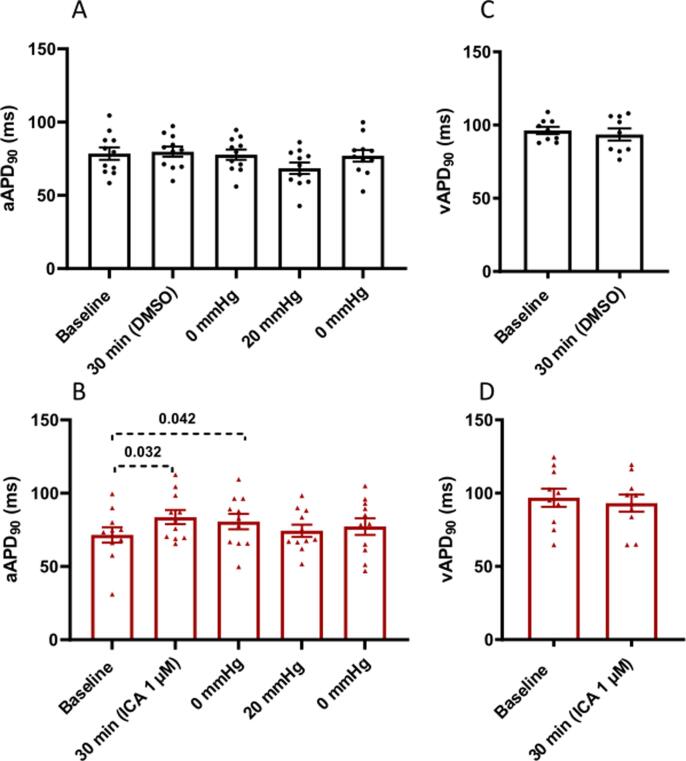
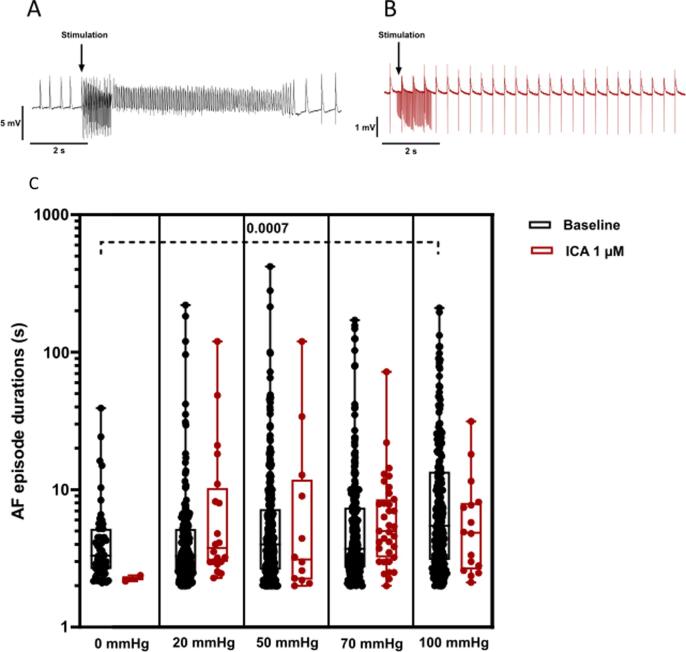
Methods: The effect of KCa2 channel inhibitor (N-(pyridin-2-yl)-4-(pyridin-2-yl)thiazol-2-amine (ICA) 1 µM) was investigated using the isolated perfused rabbit heart preparation. To stretch the left atrium (LA) a balloon was inserted and inflated. AERP and action potential duration (APD) were recorded before and after atrial stretch. AF was induced by burst pacing the LA at different degrees of atrial stretch.
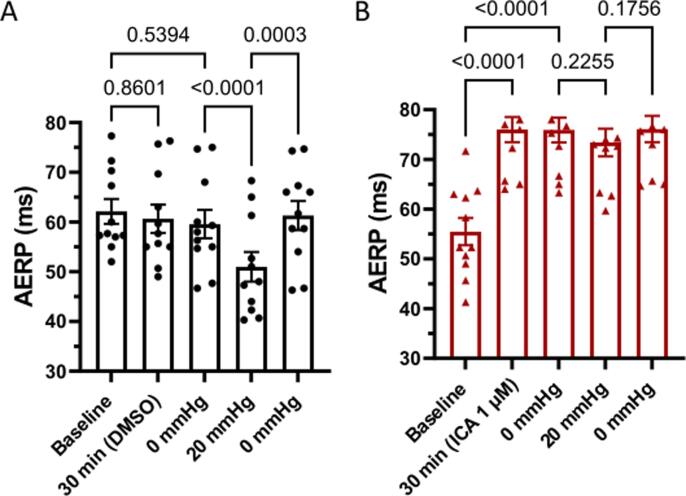
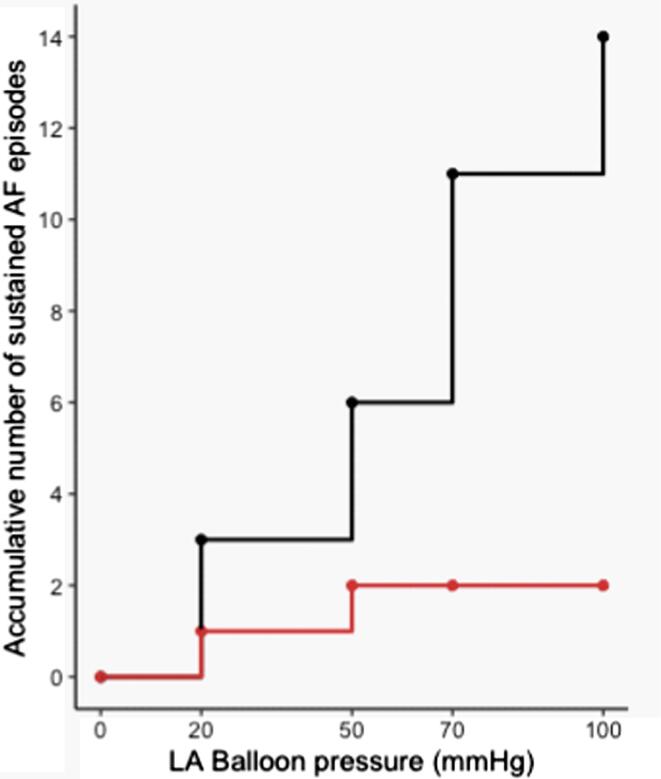
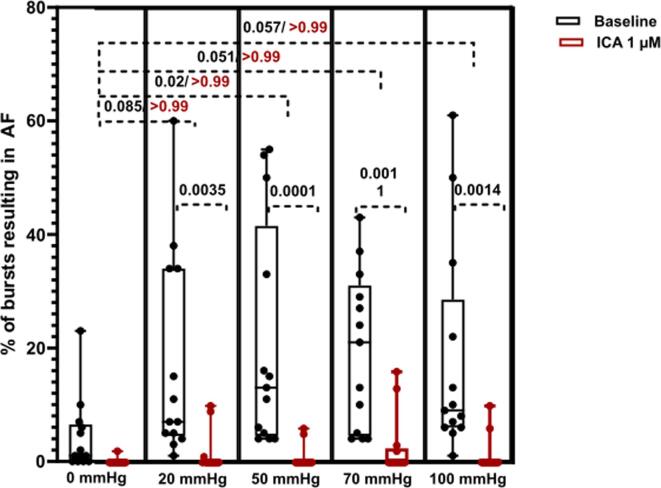
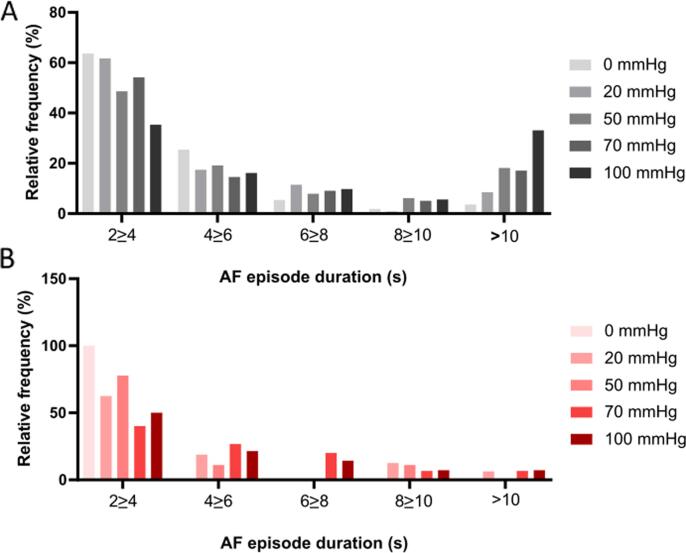
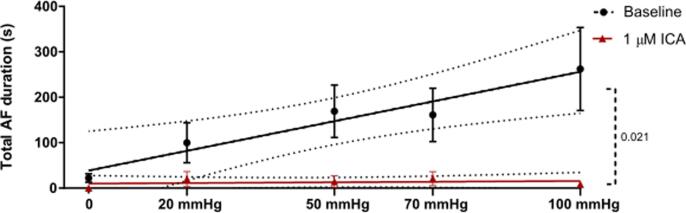
Results: Stretching of the LA by increasing the balloon pressure from 0 to 20 mmHg shortened the AERP by 8.6 ± 1 ms. In comparison, the KCa2 inhibitor ICA significantly attenuated the stretch induced shortening of AERP to 2.5 ± 1.1 ms. Total AF duration increased linearly with atrial balloon pressure. This relationship was not found in the presence of ICA. ICA lowered the incidence of AF induction and total AF duration.
Conclusion: The KCa2 channel inhibitor ICA attenuates the acute stretch induced shortening of AERP and decreases stretch induced vulnerability to AF.
Keywords: Atrial fibrillation; Ion channel; KCa2; Pharmacology; SK channel; Stretch.
© 2021 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Comment in
-
Stretching the limits of antiarrhythmic drug therapy: The promise of small-conductance calcium-activated potassium channel blockers.Int J Cardiol Heart Vasc. 2021 Dec 1;37:100924. doi: 10.1016/j.ijcha.2021.100924. eCollection 2021 Dec. Int J Cardiol Heart Vasc. 2021. PMID: 34917752 Free PMC article. No abstract available.
References
-
- Benjamin E.J., Muntner P., Alonso A. Heart Disease and stroke statistics-2019 update: a report from the American heart association. Circulation. 2019;139(10):e56–e528. - PubMed
-
- Eckstein J., Verheule S., de Groot N.M., de Groot N., Allessie M., Schotten U. Mechanisms of perpetuation of atrial fibrillation in chronically dilated atria. Prog. Biophys. Mol. Biol. 2008;97(2–3):435–451. - PubMed
-
- Ravelli F., Allessie M. Effects of atrial dilatation on refractory period and vulnerability to atrial fibrillation in the isolated Langendorff-perfused rabbit heart. Circulation. 1997;96(5):1686–1695. - PubMed
-
- Huang J.-L., Tai C.-T., Chen J.-T. Effect of atrial dilatation on electrophysiologic properties and inducibility of atrial fibrillation. Basic Res. Cardiol. 2003;98(1):16–24. - PubMed
-
- H. Calkins, R. el-Atassi, S. Kalbfleisch, J. Langberg, F. Morady, Effects of an acute increase in atrial pressure on atrial refractoriness in humans, Pacing Clin. Electrophysiol. 15(11 Pt 1) (1992) 1674–1680. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
