

CADM1 and SPC25 Gene Mutations in Lung Cancer Patients With Idiopathic Pulmonary Fibrosis
- PMID: 34746885
- PMCID: PMC8551854
- DOI: 10.1016/j.jtocrr.2021.100232
CADM1 and SPC25 Gene Mutations in Lung Cancer Patients With Idiopathic Pulmonary Fibrosis
Abstract
Introduction: To investigate the genomic profiles of patients with lung cancer with idiopathic pulmonary fibrosis (IPF-LC), mechanism of carcinogenesis, and potential therapeutic targets.
Methods: We analyzed 29 matched, surgically resected, cancerous and noncancerous lung tissues (19 IPF-LC and 10 non-IPF-LC) by whole-exome sequencing and bioinformatics analysis and established a medical-engineering collaboration with the Department of Engineering of the Tokyo University of Science.
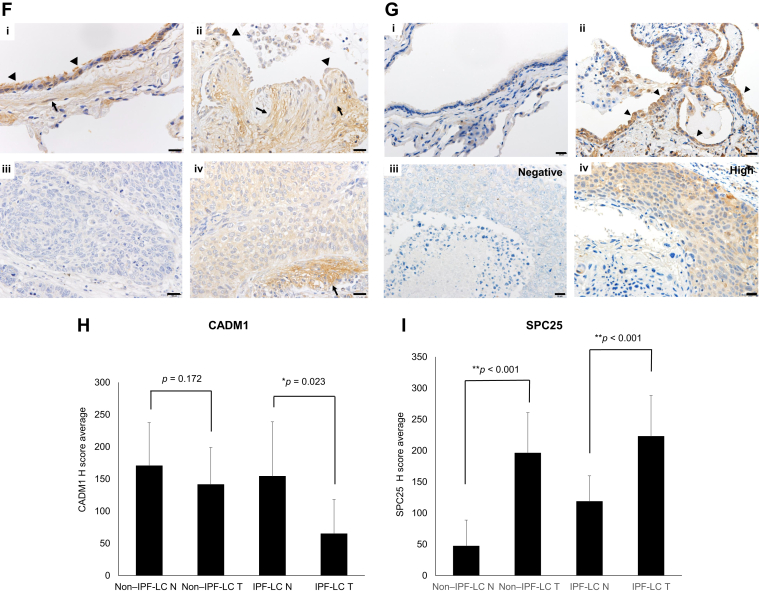
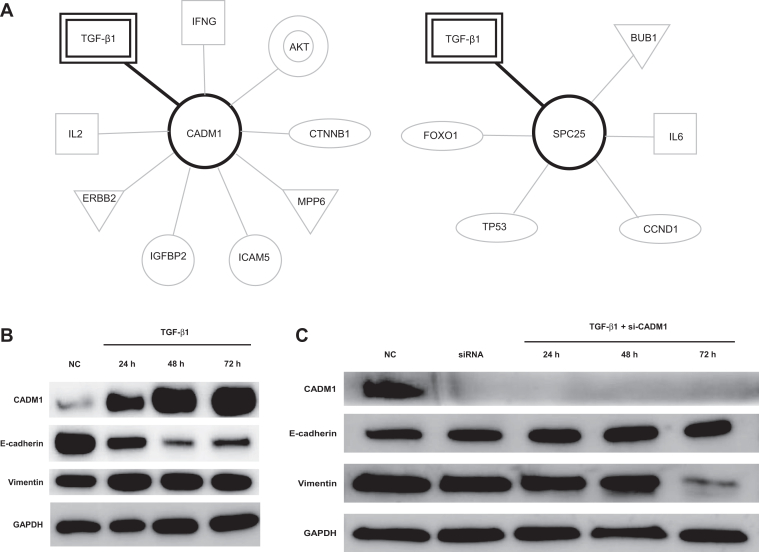
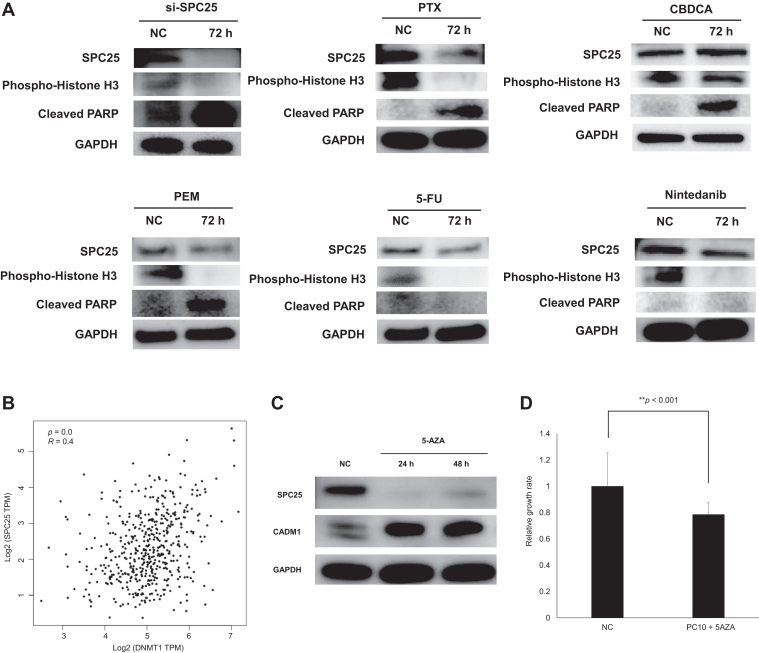
Results: In IPF-LC, CADM1 and SPC25 were mutated at a frequency of 47% (9 of 19) and 53% (10 of 19), respectively. Approximately one-third of the IPF-LC cases (7 of 19; 36%) had both mutations. Pathway analysis revealed that these two genes are involved in transforming growth factor-β1 signaling. CADM1 and SPC25 gene mutations decreased the expression of CADM1 and increased that of SPC25 revealing transforming growth factor-β1-induced epithelial-to-mesenchymal transition and cell proliferation in lung cancer cells. Furthermore, treatment with paclitaxel and DNMT1 inhibitor suppressed SPC25 expression.
Conclusions: CADM1 and SPC25 gene mutations may be novel diagnostic markers and therapeutic targets for IPF-LC.
Keywords: CADM1; Idiopathic pulmonary fibrosis; Lung cancer; SPC25; Whole-exome sequencing.
© 2021 by the International Association for the Study of Lung Cancer.
Figures





References
-
- Ozawa Y., Suda T., Naito T. Cumulative incidence of and predictive factors for lung cancer in IPF. Respirology. 2009;14:723–728. - PubMed
-
- Tomassetti S., Gurioli C., Ryu J.H. The impact of lung cancer on survival of idiopathic pulmonary fibrosis. Chest. 2015;147:157–164. - PubMed
-
- Fukuizumi A., Minegishi Y., Omori M. Weekly paclitaxel in combination with carboplatin for advanced non-small-cell lung cancer complicated by idiopathic interstitial pneumonias: a single-arm phase II study. Int J Clin Oncol. 2019;24:1543–1548. - PubMed
-
- Minegishi Y., Kuribayashi H., Kitamura K. The feasibility study of carboplatin plus etoposide for advanced small cell lung cancer with idiopathic interstitial pneumonias. J Thorac Oncol. 2011;6:801–807. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
