

Oral Anticoagulants in the Oldest Old with Recent Stroke and Atrial Fibrillation
- PMID: 34747514
- PMCID: PMC9300111
- DOI: 10.1002/ana.26267
Oral Anticoagulants in the Oldest Old with Recent Stroke and Atrial Fibrillation
Abstract
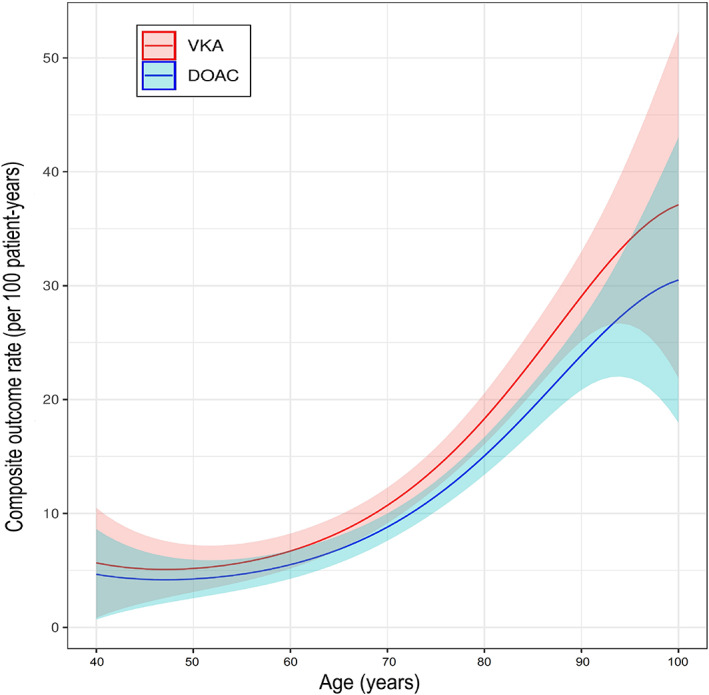
Objective: To investigate the safety and effectiveness of direct oral anticoagulants (DOAC) versus vitamin K antagonists (VKA) after recent stroke in patients with atrial fibrillation (AF) aged ≥85 years.
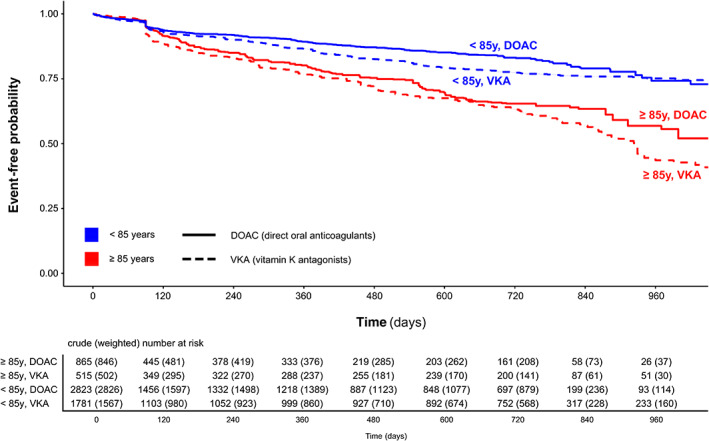
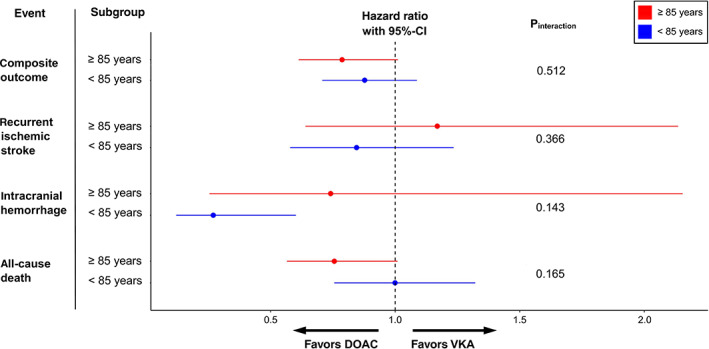
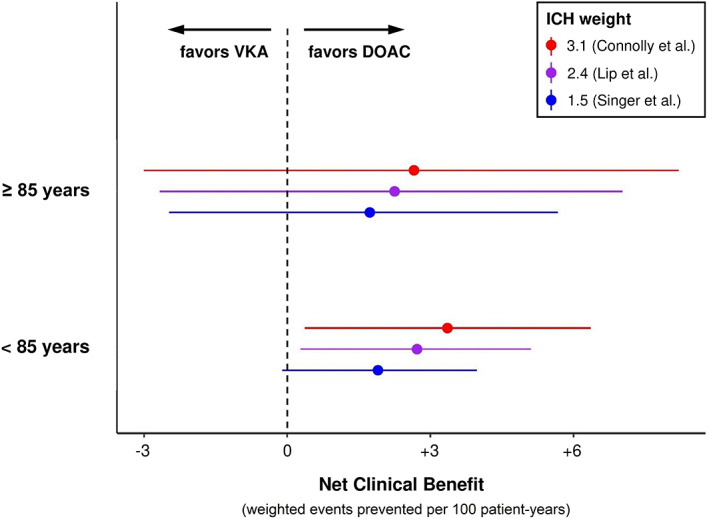
Methods: Individual patient data analysis from seven prospective stroke cohorts. We compared DOAC versus VKA treatment among patients with AF and recent stroke (<3 months) aged ≥85 versus <85 years. Primary outcome was the composite of recurrent stroke, intracranial hemorrhage (ICH) and all-cause death. We used simple, adjusted, and weighted Cox regression to account for confounders. We calculated the net benefit of DOAC versus VKA by balancing stroke reduction against the weighted ICH risk.
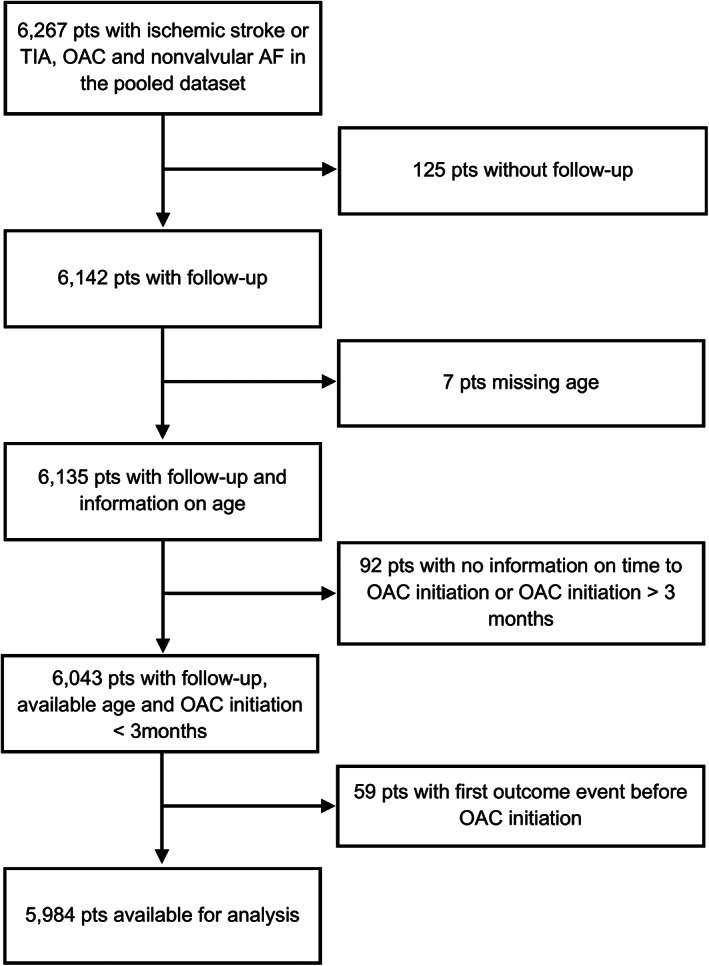
Results: In total, 5,984 of 6,267 (95.5%) patients were eligible for analysis. Of those, 1,380 (23%) were aged ≥85 years and 3,688 (62%) received a DOAC. During 6,874 patient-years follow-up, the impact of anticoagulant type (DOAC versus VKA) on the hazard for the composite outcome did not differ between patients aged ≥85 (HR≥85y = 0.65, 95%-CI [0.52, 0.81]) and < 85 years (HR<85y = 0.79, 95%-CI [0.66, 0.95]) in simple (pinteraction = 0.129), adjusted (pinteraction = 0.094) or weighted (pinteraction = 0.512) models. Analyses on recurrent stroke, ICH and death separately were consistent with the primary analysis, as were sensitivity analyses using age dichotomized at 90 years and as a continuous variable. DOAC had a similar net clinical benefit in patients aged ≥85 (+1.73 to +2.66) and < 85 years (+1.90 to +3.36 events/100 patient-years for ICH-weights 1.5 to 3.1).
Interpretation: The favorable profile of DOAC over VKA in patients with AF and recent stroke was maintained in the oldest old. ANN NEUROL 2022;91:78-88.
© 2021 The Authors. Annals of Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
MP: speaker honoraria from Sanofi‐Aventis, Boehringer‐Ingelheim, Bayer, BMS, Daiichi‐Sankyo, Pfizer (all manufacturers of anticoagulants). MK: speaker honoraria from Bayer, Nippon Boehringer‐Ingelheim, Daiichi‐Sankyo. MC: consulting fees from Boehringer‐Ingelheim, Pfizer/BMS; advisory board Daiichi‐Sankyo. GMDM: consultant/speaker honoraria from Bayer, travel honoraria from Pfizer. ST: travel grants from BMS/Pfizer. GYHL: Consultant and speaker for BMS/Pfizer, Boehringer‐Ingelheim and Daiichi‐Sankyo; no fees are received personally. LHB: consultancy or advisory board fees or speaker's honoraria from Bayer and BMS. PAL: research grants from Bayer, travel grants from Bayer, Pfizer, advisory board compensation from Bayer, Pfizer, Daiichi‐Sankyo, BMS. KT: lecture honoraria (modest) from Daiichi‐Sankyo, Bayer Yakuhin, Nippon Boehringer‐Ingelheim, BMS. DJW: personal fees from Bayer, Portola (manufacturer of the anticoagulant reversal agent andexanet alfa). STE: research support from Pfizer, Daiichi‐Sankyo; compensation from Stago (manufacturer of coagulation testing systems) for educational material; travel/speaker honoraria from Bayer, Boehringer‐Ingelheim, BMS, Daiichi‐Sankyo; advisory board Bayer, Boehringer‐Ingelheim, BMS. The remaining authors declare no relevant conflicts.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics–2015 update: a report from the American Heart Association. Circulation 2015;131:e29–e322. - PubMed
-
- Gabet A, Guenancia C, Duloquin G, et al. Ischemic stroke with atrial fibrillation: characteristics and time trends 2006 to 2017 in the Dijon stroke registry. Stroke 2021;52:2077–2085. - PubMed
-
- Kleindorfer DO, Towfighi A, Chaturvedi S, et al. 2021 guideline for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline from the American Heart Association/American Stroke Association. Stroke 2021;52:e364–e467. - PubMed
-
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta‐analysis of randomised trials. Lancet 2014;383:955–962. - PubMed
-
- Lauw MN, Eikelboom JW, Coppens M, et al. Effects of dabigatran according to age in atrial fibrillation. Heart 2017;103:1015–1023. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- Italian Ministery of Heatlh Ricerca Corrente IRCCS MultiMedica
- Stroke Fund and Scientific Fund of the University Hospital Basel, Switzerland
- Intramural Research Fund (H28-4-1)/National Cerebral and Cardiovascular Center
- Daiichi Sankyo AG (Switzerland)
- CS/17/6/33361/BHF_/British Heart Foundation/United Kingdom
- MR/N003403/1/MRC_/Medical Research Council/United Kingdom
- Bayer AG (Switzerland)
- Grant-in-Aid (H23-Junkanki-Ippan-010)/Ministry of Health, Labour and Welfare
- British Stroke Association
- Science Fund Rehabilitation of the University Department of Geriatric Medicine Felix Platter Basel, Switzerland
- Intramural Research Fund (H23-4-3)/National Cerebral and Cardiovascular Center
- Swiss Heart Foundation
