

Assessing patent ductus arteriosus in preterm infants from standard neonatal intensive care monitoring
- PMID: 34748081
- PMCID: PMC8897357
- DOI: 10.1007/s00431-021-04311-9
Assessing patent ductus arteriosus in preterm infants from standard neonatal intensive care monitoring
Abstract
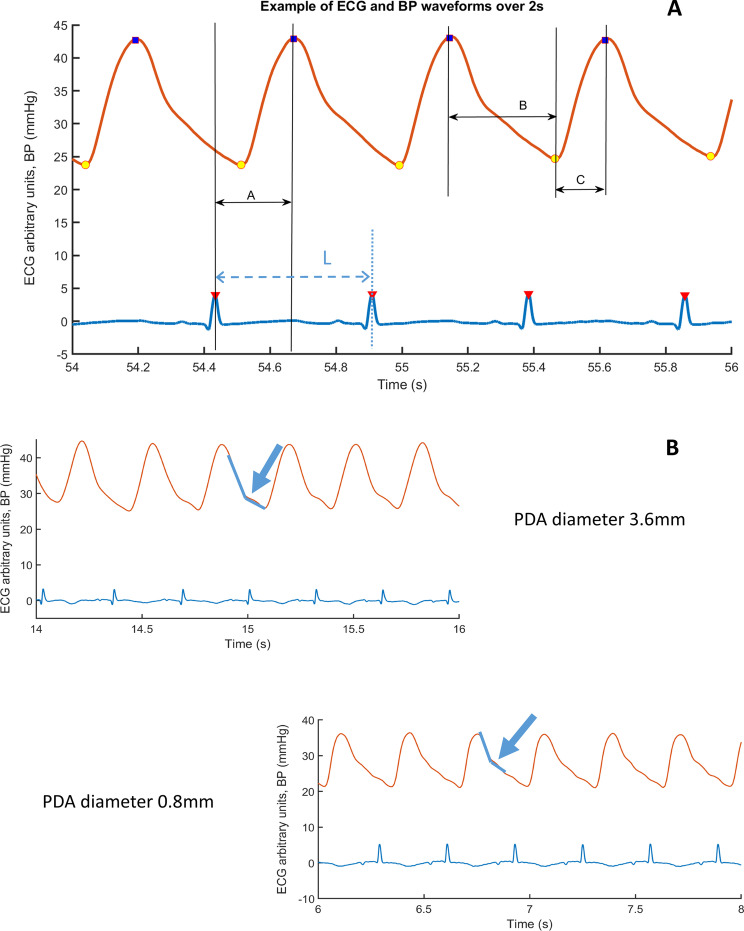
Monitoring patent ductus arteriosus (PDA) in premature infants is currently performed intermittently using echocardiography which requires considerable expertise. The aim of this pilot study was to investigate whether PDA status could be assessed from standard neonatal intensive care monitoring. Electrocardiography (ECG) and blood pressure (BP) waveforms were acquired from extremely preterm infants using standard neonatal monitors. We developed software using MATLAB to analyse ECG and BP waveforms and their interrelationships in terms of pulse transit time (PTT) and pulse wave velocity (PWV). The times from peak systolic BP to diastolic trough (BPFt) and from the diastolic trough to peak systolic BP (BPRt) were also calculated. PTT, BPFt and BPRt were normalised for heart rate (HR) termed NPTT, NBPFt and NBPRt, respectively. ECG, invasive aortic BP monitoring and echocardiography were performed in 14 preterm infants < 29 weeks' gestation in the first 3 days after birth. The median (range) birth weight of the infants was 0.90 (0.48-1.31) kg, gestation 26.6 (24.0-28.7) weeks, PDA diameter 1.6 (0.8-3.6) mm and mean BP 32 (16-40) mmHg. We found a significant positive correlation between PDA diameter and NPTT (r = 0.69, P = 0.007) as well as NBPFt (r = 0.65, P = 0.012) and NBPRt (r = 0.71, P = 0.005). No relationship was found between PDA diameter and pulse pressure.Conclusions: Interrelationships between ECG and BP traces as well as BP waveform time analysis are straightforward to measure and associated with PDA diameter. The results of this pilot study suggest that this approach may help provide biomarkers for continuous monitoring PDA diameter and function. What is Known: • Patent ductus arteriosus (PDA) in premature infants is associated with increased risk of developing chronic lung disease, necrotising enterocolitis and cerebral injury. • Currently PDA is assessed intermittently using echocardiography which requires considerable expertise and sometimes is not well tolerated by critically ill preterm infants. What is New: • Blood pressure (BP) and ECG waveform interrelation and BP trace time analysis, taking account of heart rate, relate to PDA diameter. • ECG and BP waveform phase difference as well as BP waveform time analysis may be useful in the continuous assessment of PDA function.
Keywords: Biomarkers; Echocardiography; Haemodynamics; Patent ductus arteriosus; Preterm infants.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
Neonatal Intensive Care Unit-Level Patent Ductus Arteriosus Treatment Rates and Outcomes in Infants Born Extremely Preterm.J Pediatr. 2020 May;220:34-39.e5. doi: 10.1016/j.jpeds.2020.01.069. Epub 2020 Mar 4. J Pediatr. 2020. PMID: 32145968
-
Change in blood pressure and pulse pressure in preterm infants after treatment of patent ductus arteriosus with indomethacin.Korean Circ J. 2011 Apr;41(4):203-8. doi: 10.4070/kcj.2011.41.4.203. Epub 2011 Apr 30. Korean Circ J. 2011. PMID: 21607171 Free PMC article.
-
Ibuprofen for the treatment of patent ductus arteriosus in preterm or low birth weight (or both) infants.Cochrane Database Syst Rev. 2020 Feb 11;2(2):CD003481. doi: 10.1002/14651858.CD003481.pub8. Cochrane Database Syst Rev. 2020. PMID: 32045960 Free PMC article.
-
Value of bedside echocardiography in predicting persistent patency of the ductus arteriosus during the early postnatal period in very low birth weight infants.Zhongguo Dang Dai Er Ke Za Zhi. 2022 Jan 15;24(1):26-32. doi: 10.7499/j.issn.1008-8830.2109087. Zhongguo Dang Dai Er Ke Za Zhi. 2022. PMID: 35177172 Free PMC article. Chinese, English.
-
[Transcatheter occlusion of patent ductus arteriosus in a preterm infant and review of literatures].Zhonghua Er Ke Za Zhi. 2016 Jan;54(1):43-6. doi: 10.3760/cma.j.issn.0578-1310.2016.01.010. Zhonghua Er Ke Za Zhi. 2016. PMID: 26791923 Review. Chinese.
Cited by
-
Serum Biomarkers in Patent Ductus Arteriosus in Preterm Infants: A Narrative Review.Biomedicines. 2025 Mar 9;13(3):670. doi: 10.3390/biomedicines13030670. Biomedicines. 2025. PMID: 40149646 Free PMC article. Review.
References
-
- Benitz WE (2016) Patent ductus arteriosus in preterm infants. Pediatric 137(1) - PubMed
-
- Ohlsson A, Walia R, Shah SS (2015) Ibuprofen for the treatment of patent ductus arteriosus in preterm or low birth weight (or both) infants. Cochrane Database Syst Rev (2):Cd003481 - PubMed
-
- Popat H, Robledo KP, Sebastian L, Evans N, Gill A, Kluckow M, et al. Interobserver agreement and image quality of functional cardiac ultrasound measures used in a randomised trial of delayed cord clamping in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2018;103(3):F257–F263. doi: 10.1136/archdischild-2016-312006. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
