

Perioperative NSAIDs and Long-Term Outcomes After cancer Surgery: a Systematic Review and Meta-analysis
- PMID: 34748112
- PMCID: PMC8575753
- DOI: 10.1007/s11912-021-01133-8
Perioperative NSAIDs and Long-Term Outcomes After cancer Surgery: a Systematic Review and Meta-analysis
Abstract
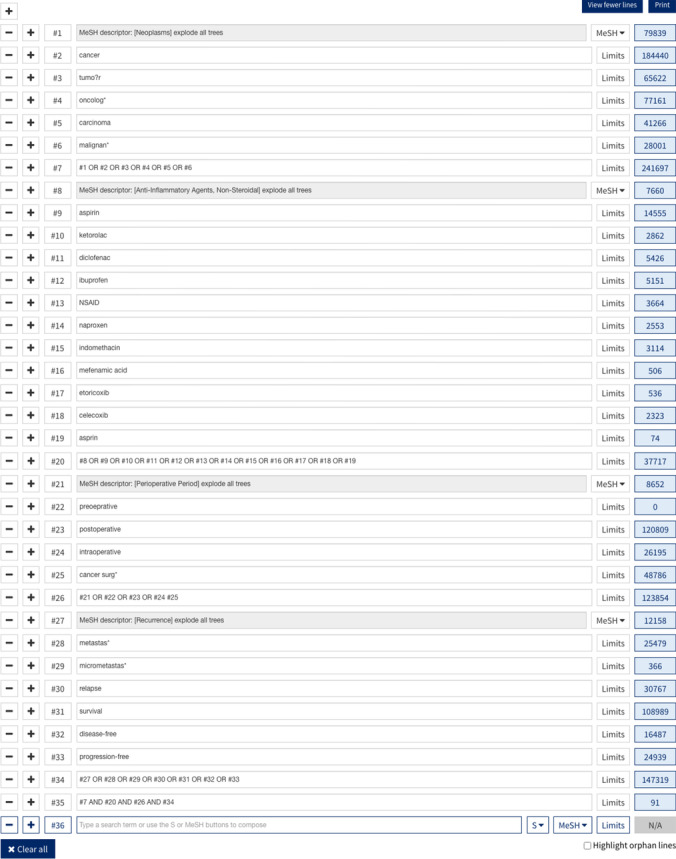
Purpose of review: This review investigated the use of perioperative non-steroidal anti-inflammatory drugs (NSAIDs) and long-term outcomes in cancer surgery patients, and whether this is dependent on cancer type, type of NSAID and timing of administration.
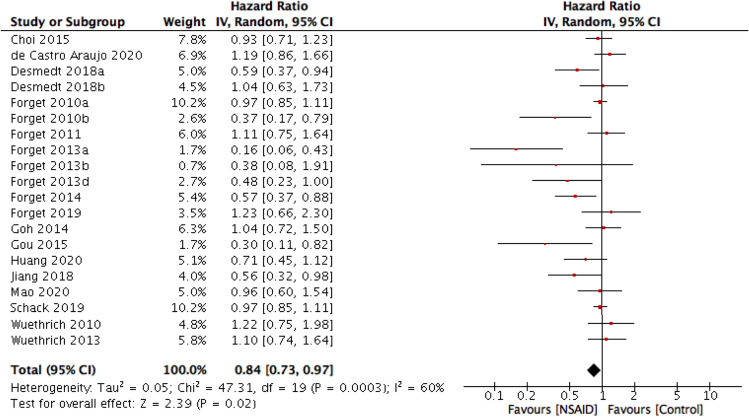
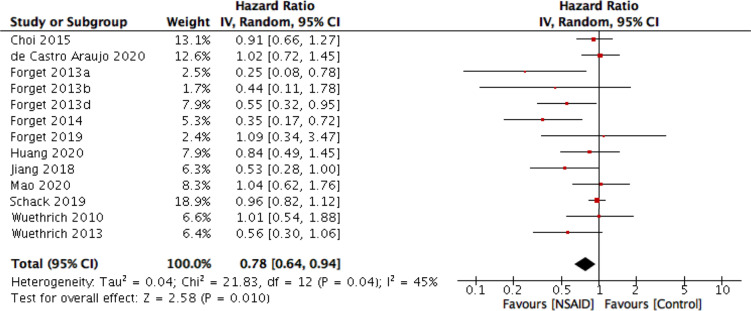
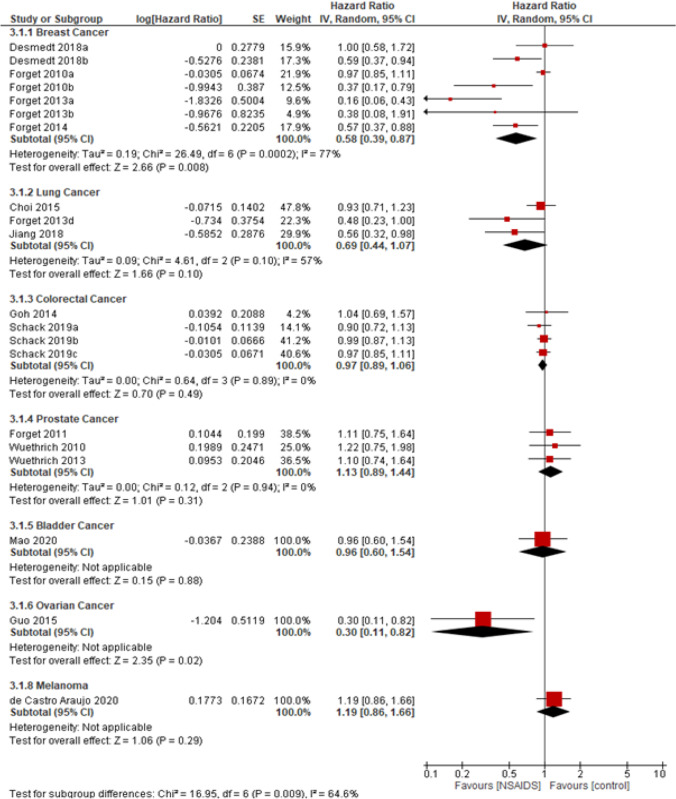
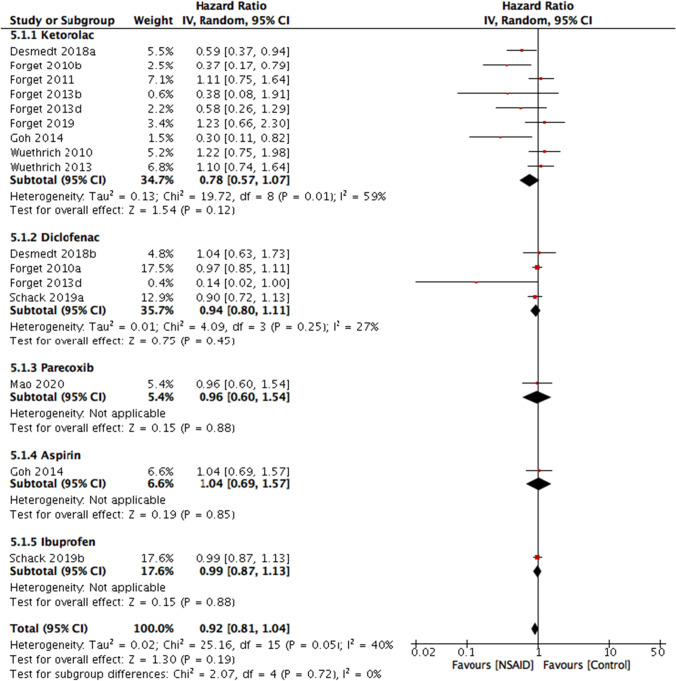
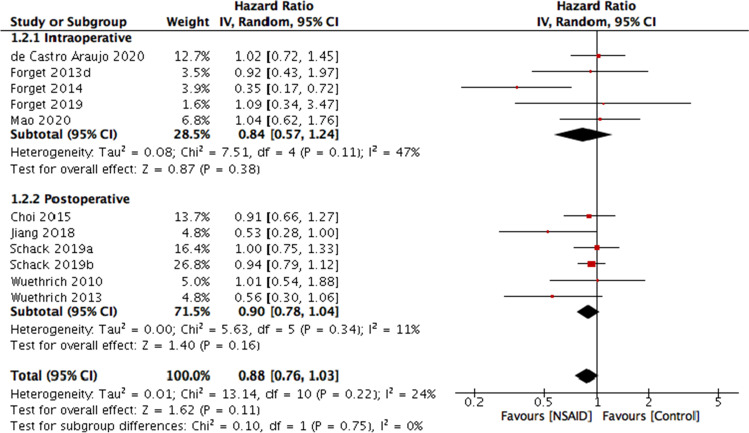
Findings: Perioperative NSAID use was found to be associated with longer disease-free survival (hazard ration, HR = 0.84 (95% CI, 0.73-0.97)) and overall survival (HR = 0.78 (95% CI, 0.64-0.94)). No difference was found between different types of NSAID for disease-free survival, although in overall survival ketorolac use was significant (HR = 0.63 (95% CI, 0.42-0.95)). Analysis on the timing of NSAID administration found no subgroup to be associated with cancer outcomes. The cancer-type analysis found an association with outcomes in breast and ovarian cancers. However, the level of certainty remains very low, mostly due to the heterogeneity and the retrospective nature of most studies. Perioperative NSAID use may be associated with increased disease-free and overall survival after cancer surgery. This may be dependent on the type of cancer and type of NSAID, and further research is needed to support this. These data may inform future prospective trials, which are needed to determine the clinical impact, as well as optimal NSAID regimen.
Keywords: Cancer; Disease-free survival; Long-term outcomes; NSAIDs; Perioperative; Surgery.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Hiller JG, Perry NJ, Poulogiannis G, Riedel B, Sloan EK. Perioperative events influence cancer recurrence risk after surgery. Nat Rev Clin Oncol. 2018;15:205–218. - PubMed
-
- Hashimoto M, Tanaka F, Yoneda K, Takuwa T, Matsumoto S, Okumura Y, et al. Significant increase in circulating tumour cells in pulmonary venous blood during surgical manipulation in patients with primary lung cancer. Interactive CardioVascular and Thoracic Surgery. 2014;18(6):775–783. - PubMed
-
- Ikeda M, Furukawa H, Imamura H, Shimizu J, Ishida H, Masutani S, et al. Surgery for gastric cancer increases plasma levels of vascular endothelial growth factor and von Willebrand factor. Gastric Cancer. 2002;5(3):137–141. - PubMed
-
- Maniwa Y, Okada M, Ishii N, Kiyooka K. Vascular endothelial growth factor increased by pulmonary surgery accelerates the growth of micrometastases in metastatic lung cancer. Chest. 1998;114(6):1668–1675. - PubMed
-
- Page GG. Surgery-induced immunosuppression and postoperative pain management. AACN clinical issues: advanced practice in acute and critical care. 2005;16(3):302–309. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
