

Safety and efficacy of esaxerenone in Japanese hypertensive patients with heart failure with reduced ejection fraction: A retrospective study
- PMID: 34748605
- PMCID: PMC8575262
- DOI: 10.1371/journal.pone.0259485
Safety and efficacy of esaxerenone in Japanese hypertensive patients with heart failure with reduced ejection fraction: A retrospective study
Abstract
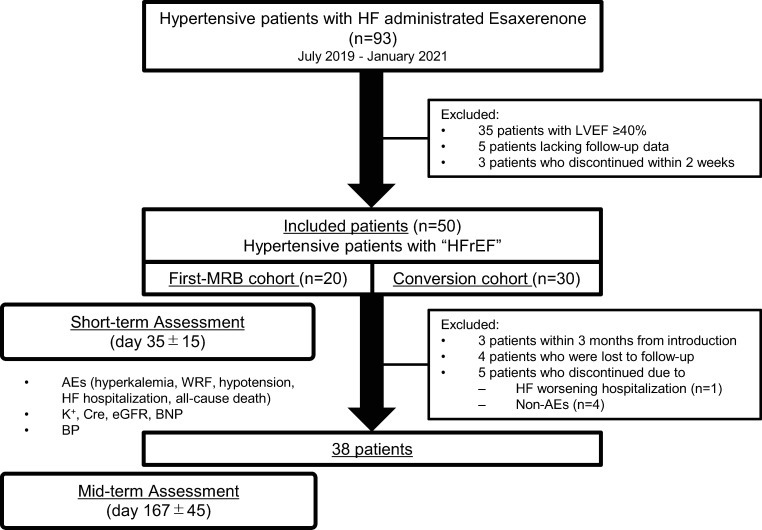
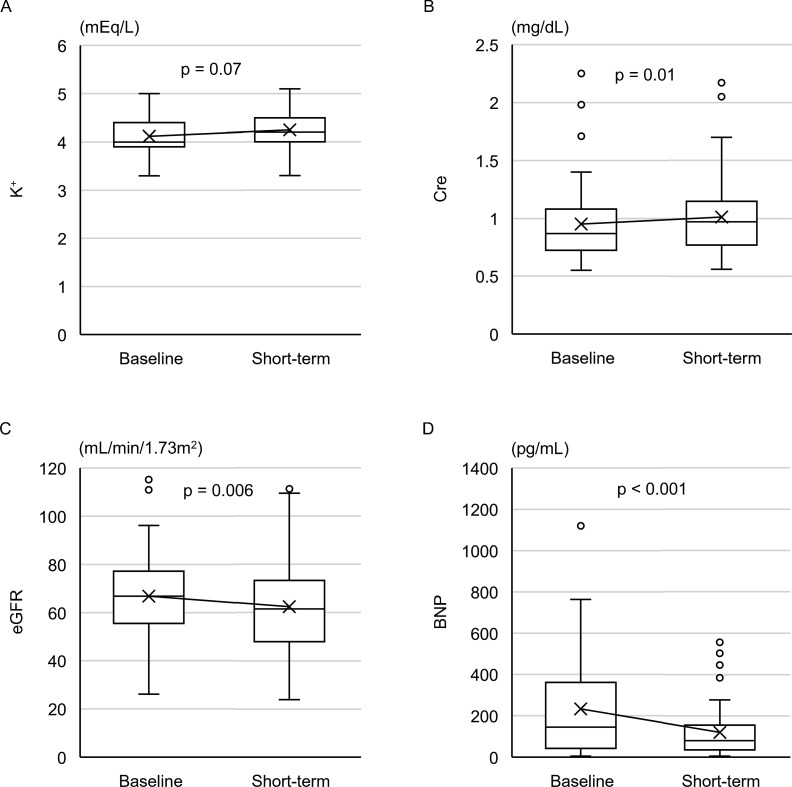
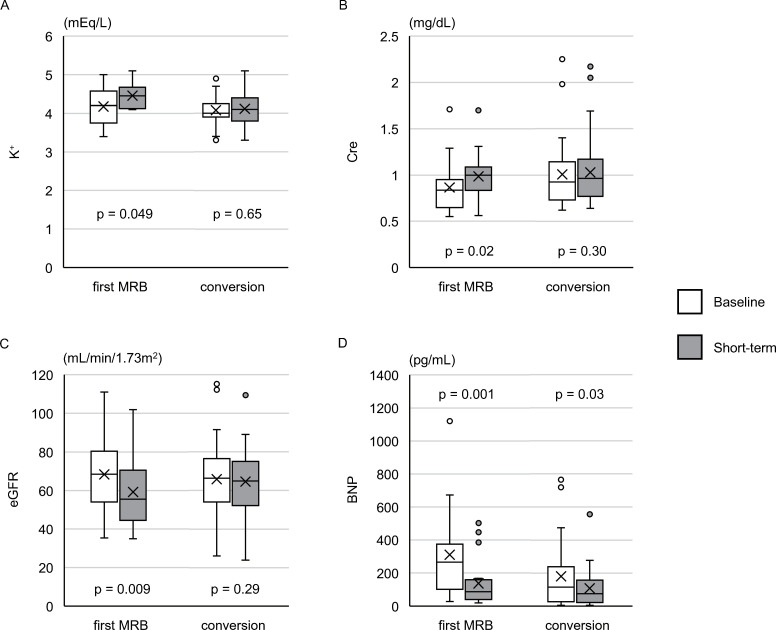
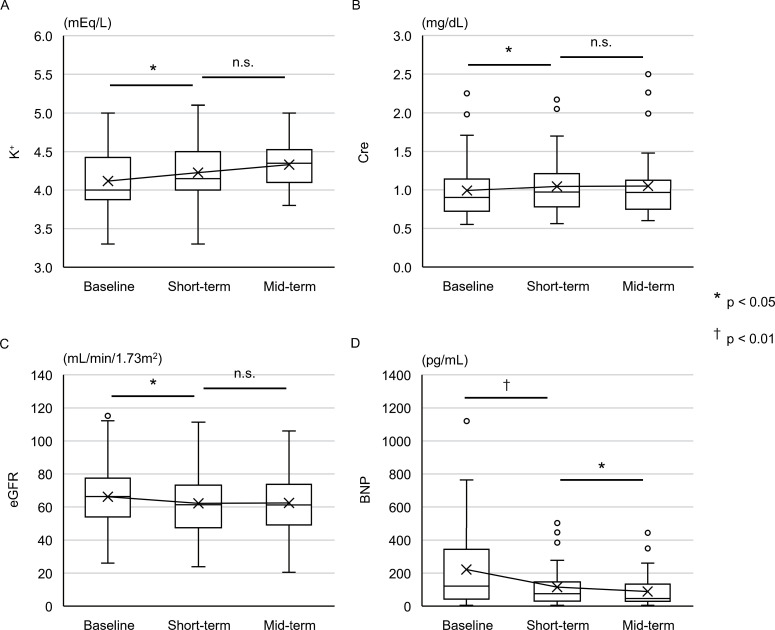
Esaxerenone, a mineralocorticoid receptor blocker (MRB), is a new antihypertensive agent. However, esaxerenone-related data with respect to hypertension with heart failure are limited. We investigated the safety and efficacy of esaxerenone in hypertensive patients with heart failure with reduced ejection fraction (HFrEF). Hypertensive patients with HFrEF treated with esaxerenone were retrospectively analyzed at two timepoints (short-term: 35±15 days; mid-term: 167±45 days). Adverse events including hyperkalemia (K+ >5.5 mEq/L), worsening renal function (WRF; estimated glomerular filtration rate (eGFR) reduction by ≥20%), and hypotension (systolic blood pressure <90 mmHg) were evaluated. eGFR and K+, serum creatinine, and brain natriuretic peptide (BNP) levels at baseline, short-term, and mid-term assessments were compared. Patients administered esaxerenone as their first MRB (first-MRB cohort) and those who converted from another MRB (conversion cohort) were separately analyzed. There were 50 (56±10 years old, 26% female) patients. At the short-term assessment, hyperkalemia or hypotension was not observed at a dose of 2.0±0.9 mg/day. Seven patients (14%) showed WRF. K+ was slightly elevated (4.12±0.41 to 4.25±0.39 mmol/L, p = 0.07) and eGFR was significantly reduced (66.9±19.6 mL/min/1.73 m2 to 62.4±19.7 mL/min/1.73 m2, p = 0.006). In the conversion cohort, significant changes in K+ and eGFR from baseline were not observed at the short-term assessment. BNP levels were consistently improved regardless of the cohorts (first-MRB cohort, 310 [110-370] pg/mL to 137 [47-152] pg/mL, p = 0.001; conversion cohort, 181 [30-203] pg/mL to 108 [26-146] pg/mL, p = 0.028). At the mid-term assessment, there were no significant changes in K+ and eGFR compared with the short-term assessment. In conclusion, esaxerenone was safe for hypertensive patients with HFrEF. Hyperkalemia and hypotension were rarely noted, while eGFR was marginally reduced. Moreover, esaxerenone might be beneficial for HFrEF in terms of BNP level reduction.
Conflict of interest statement
We declared that YK received lecture fees and research grant from Daiichi Sankyo Co., Ltd. YK does not have any other relation with this funder, including employment, consultancy, patents, products in development, or marketed products. This does not influence our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Carey RM, Calhoun DA, Bakris GL, Brook RD, Daugherty SL, Dennison-Himmelfarb CR, et al.. Resistant Hypertension: Detection, Evaluation, and Management: A Scientific Statement From the American Heart Association. Hypertension. 2018;72(5):e53–e90. doi: 10.1161/HYP.0000000000000084 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
