

Multiscale heterogeneity in gastric adenocarcinoma evolution is an obstacle to precision medicine
- PMID: 34749812
- PMCID: PMC8576943
- DOI: 10.1186/s13073-021-00975-y
Multiscale heterogeneity in gastric adenocarcinoma evolution is an obstacle to precision medicine
Abstract
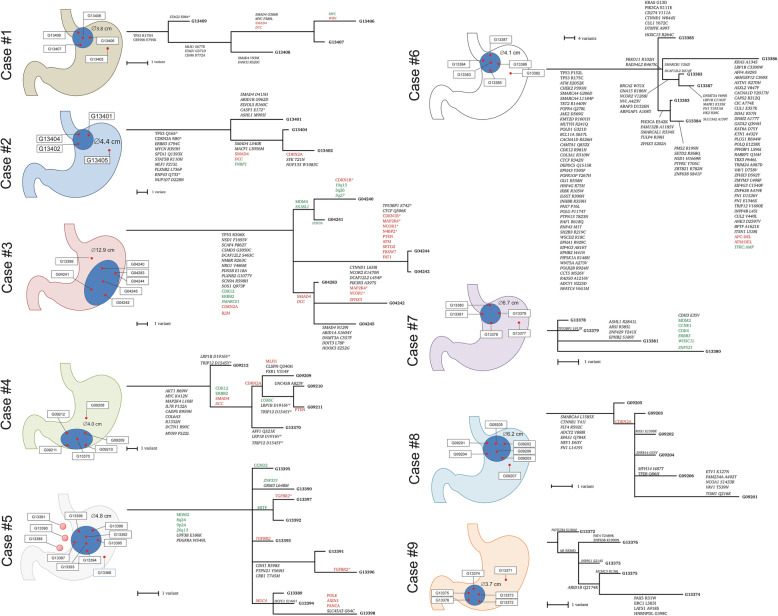
Background: Cancer is a somatic evolutionary disease and adenocarcinomas of the stomach and gastroesophageal junction (GC) may serve as a two-dimensional model of cancer expansion, in which tumor subclones are not evenly mixed during tumor progression but rather spatially separated and diversified. We hypothesize that precision medicine efforts are compromised when clinical decisions are based on a single-sample analysis, which ignores the mechanisms of cancer evolution and resulting intratumoral heterogeneity. Using multiregional whole-exome sequencing, we investigated the effect of somatic evolution on intratumoral heterogeneity aiming to shed light on the evolutionary biology of GC.
Methods: The study comprised a prospective discovery cohort of 9 and a validation cohort of 463 GCs. Multiregional whole-exome sequencing was performed using samples form 45 primary tumors and 3 lymph node metastases (range 3-10 tumor samples/patient) of the discovery cohort.
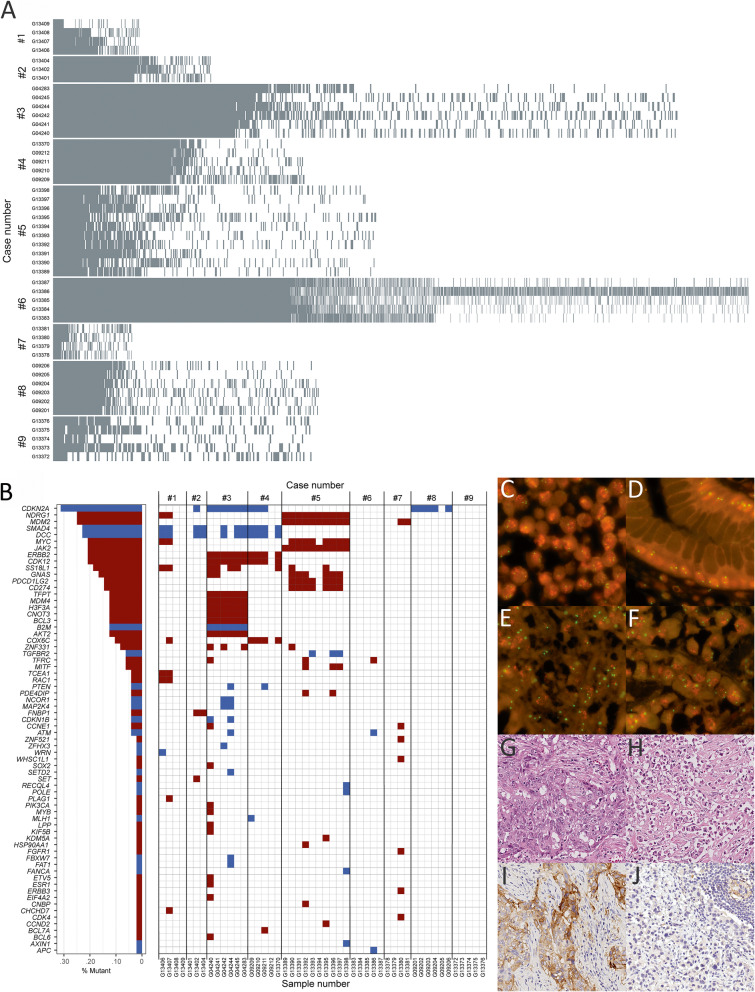
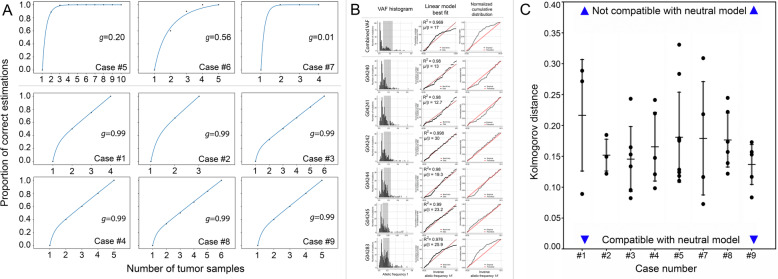
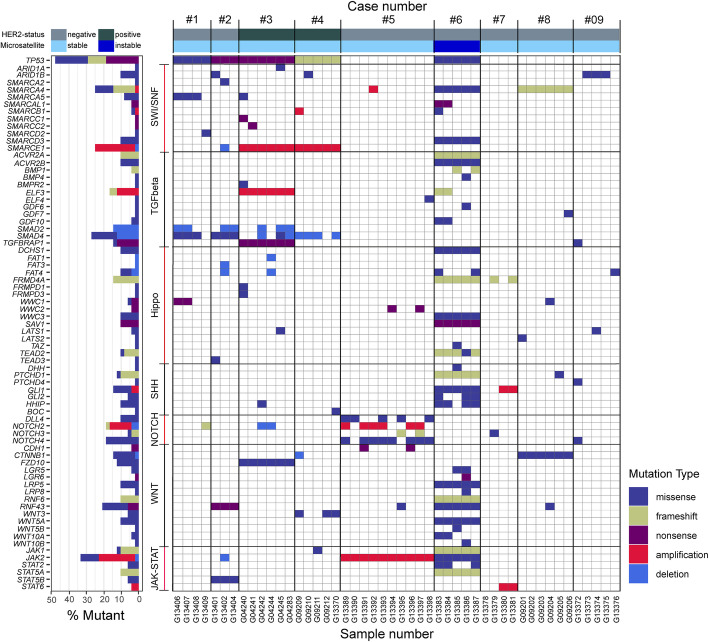
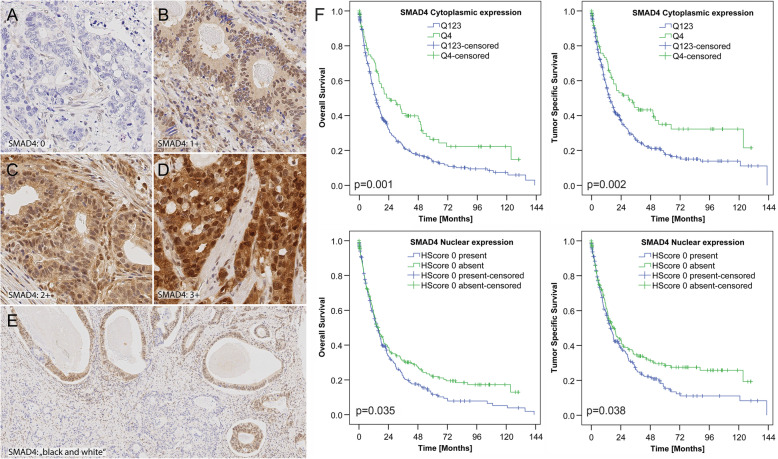
Results: In total, the discovery cohort harbored 16,537 non-synonymous mutations. Intratumoral heterogeneity of somatic mutations and copy number variants were present in all tumors of the discovery cohort. Of the non-synonymous mutations, 53-91% were not present in each patient's sample; 399 genes harbored 2-4 different non-synonymous mutations in the same patient; 175 genes showed copy number variations, the majority being heterogeneous, including CD274 (PD-L1). Multi-sample tree-based analyses provided evidence for branched evolution being most complex in a microsatellite instable GC. The analysis of the mode of evolution showed a high degree of heterogeneity in deviation from neutrality within each tumor. We found evidence of parallel evolution and evolutionary trajectories: different mutations of SMAD4 aligned with different subclones and were found only in TP53 mutant GCs.
Conclusions: Neutral and non-neutral somatic evolution shape the mutational landscape in GC along its lateral expansions. It leads to complex spatial intratumoral heterogeneity, where lymph node metastases may stem from different areas of the primary tumor, synchronously. Our findings may have profound effects on future patient management. They illustrate the risk of mis-interpreting tumor genetics based on single-sample analysis and open new avenues for an evolutionary classification of GC, i.e., the discovery of distinct evolutionary trajectories which can be utilized for precision medicine.
Keywords: Evolution; Gastric cancer; Intratumoral heterogeneity; SMAD4; TP53.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Lee J, Kim ST, Kim K, Lee H, Kozarewa I, Mortimer PGS, Odegaard JI, Harrington EA, Lee J, Lee T, Oh SY, Kang JH, Kim JH, Kim Y, Ji JH, Kim YS, Lee KE, Kim J, Sohn TS, An JY, Choi MG, Lee JH, Bae JM, Kim S, Kim JJ, Min YW, Min BH, Kim NKD, Luke S, Kim YH, Hong JY, Park SH, Park JO, Park YS, Lim HY, Talasaz A, Hollingsworth SJ, Kim KM, Kang WK. Tumor genomic profiling guides patients with metastatic gastric cancer to targeted treatment: the VIKTORY Umbrella Trial. Cancer Discov. 2019;9(10):1388–1405. doi: 10.1158/2159-8290.CD-19-0442. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
