

First-line Nivolumab plus Ipilimumab Versus Sunitinib in Patients Without Nephrectomy and With an Evaluable Primary Renal Tumor in the CheckMate 214 Trial
- PMID: 34750035
- PMCID: PMC10202028
- DOI: 10.1016/j.eururo.2021.10.001
First-line Nivolumab plus Ipilimumab Versus Sunitinib in Patients Without Nephrectomy and With an Evaluable Primary Renal Tumor in the CheckMate 214 Trial
Abstract
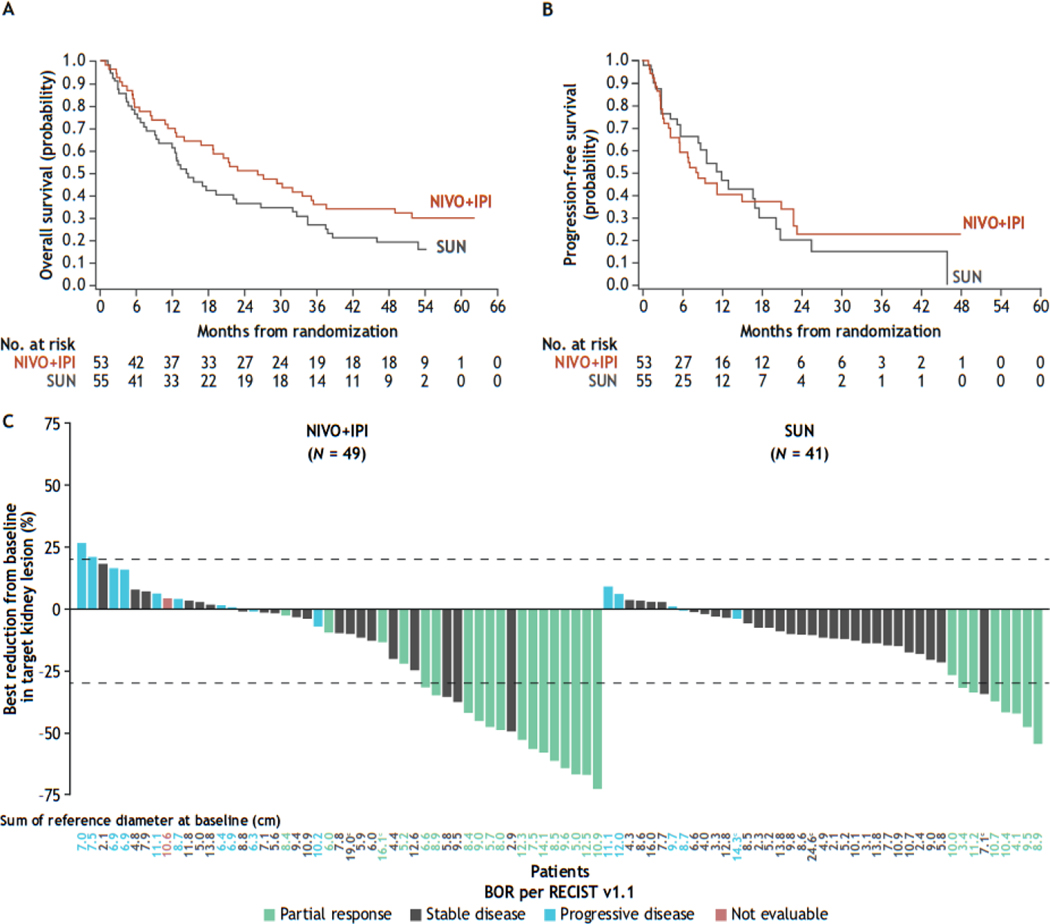
We present an exploratory post hoc analysis from the phase 3 CheckMate 214 trial of first-line nivolumab plus ipilimumab (NIVO+IPI) versus sunitinib in a subgroup of 108 patients with advanced renal cell carcinoma (aRCC) without prior nephrectomy and with an evaluable primary tumor, a population under-represented in clinical trials. Patients with clear cell aRCC were randomized to NIVO+IPI every 3 wk for four doses followed by NIVO monotherapy, or sunitinib every day for 4 wk (6-wk cycle). Overall survival (OS), progression-free survival (PFS), objective response rate (ORR), and primary tumor shrinkage were assessed. PFS and ORR were assessed per independent radiology review committee using RECIST version 1.1. With minimum study follow-up of 4 yr for intent-to-treat patients, OS favored NIVO+IPI (n = 53) over sunitinib (n = 55; hazard ratio 0.63, 95% confidence interval 0.40-1.0) among patients without prior nephrectomy. ORR was higher (34% vs 15%; p = 0.0041) and median duration of response was longer with NIVO+IPI versus sunitinib (20.5 vs 14.1 mo); the best overall response was partial response in either arm. A ≥30% reduction in the diameter of intact target renal tumors was achieved in 35% of patients with NIVO+IPI versus 20% with sunitinib. Safety was consistent with the global study population. In conclusion, in patients with aRCC without prior nephrectomy and with an evaluable primary tumor, NIVO+IPI showed survival benefits and renal tumor reduction versus sunitinib. This trial is registered at ClinicalTrials.gov as NCT02231749. PATIENT SUMMARY: In an exploratory analysis of a large global trial (CheckMate 214), we observed positive outcomes (both survival and tumor response to treatment) with nivolumab plus ipilimumab over sunitinib in a subgroup of patients with advanced kidney cancer who did not undergo removal of their primary kidney tumor. This subset of patients represents a population that has not been studied in clinical trials and for whom outcomes with new immunotherapy combination regimens are not yet known. We conclude that treatment with nivolumab plus ipilimumab offers these patients a survival benefit versus sunitinib, consistent with that observed in the overall study, as well as a notable kidney tumor reduction.
Keywords: Advanced renal cell carcinoma; CheckMate 214; Cytoreductive nephrectomy; Ipilimumab; Nivolumab.
Copyright © 2021 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
Comment in
-
"Immune-Cell Pawns" Plot Promotion and Corner Kidney Cancer: CheckMate 214.Eur Urol. 2022 Mar;81(3):272-273. doi: 10.1016/j.eururo.2021.11.006. Epub 2021 Nov 24. Eur Urol. 2022. PMID: 34838352 No abstract available.
-
Exploratory results from the CheckMate 214 trial.Nat Rev Urol. 2022 Jan;19(1):4. doi: 10.1038/s41585-021-00553-2. Nat Rev Urol. 2022. PMID: 34887568 No abstract available.
-
Urological Oncology: Adrenal, Renal, Ureteral and Retroperitoneal Tumors.J Urol. 2023 Feb;209(2):442-443. doi: 10.1097/JU.0000000000003058. Epub 2022 Nov 16. J Urol. 2023. PMID: 36382504 No abstract available.
References
-
- Donskov F, Xie W, Overby A, et al. Synchronous versus metachronous metastatic disease: Impact of time to metastasis on patient outcome-results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur Urol Oncol 2020;3:530–9. - PubMed
-
- Courcier J, Dalban C, Laguerre B, et al. Primary renal tumour response in patients treated with nivolumab for metastatic renal cell carcinoma: results from the GETUG-AFU 26 NIVOREN trial. Eur Urol 2021;80:325–9. - PubMed
-
- Méjean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal-cell carcinoma. N Engl J Med 2018;379:417–27. - PubMed
-
- Tannir NM, Powles T, Escudier B, et al. Clinical outcomes by nephrectomy status in METEOR, a randomized phase 3 trial of cabozantinib versus everolimus in patients with advanced renal cell carcinoma. Kidney Cancer 2020;4:29–39.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
