

Anatomic accuracy, physiologic characteristics, and fidelity of very low birth weight infant airway simulators
- PMID: 34750523
- PMCID: PMC8573578
- DOI: 10.1038/s41390-021-01823-w
Anatomic accuracy, physiologic characteristics, and fidelity of very low birth weight infant airway simulators
Abstract
Background: Medical simulation training requires realistic simulators with high fidelity. This prospective multi-center study investigated anatomic precision, physiologic characteristics, and fidelity of four commercially available very low birth weight infant simulators.
Methods: We measured airway angles and distances in the simulators Premature AirwayPaul (SIMCharacters), Premature Anne (Laerdal Medical), Premie HAL S2209 (Gaumard), and Preterm Baby (Lifecast Body Simulation) using computer tomography and compared these to human cadavers of premature stillbirths. The simulators' physiologic characteristics were tested, and highly experienced experts rated their physical and functional fidelity.
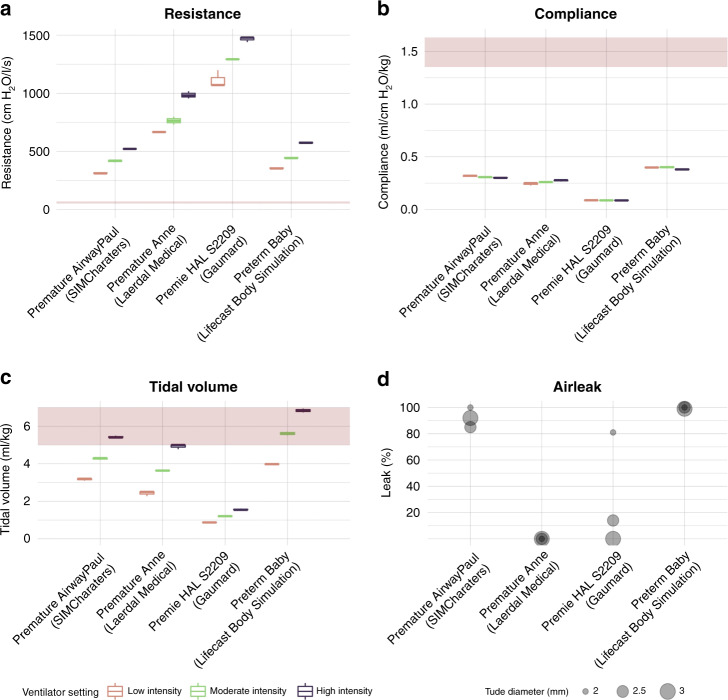
Results: The airway angles corresponded to those of the reference cadavers in three simulators. The nasal inlet to glottis distance and the mouth aperture to glottis distance were only accurate in one simulator. All simulators had airway resistances up to 20 times higher and compliances up to 19 times lower than published reference values. Fifty-six highly experienced experts gave three simulators (Premature AirwayPaul: 5.1 ± 1.0, Premature Anne 4.9 ± 1.1, Preterm Baby 5.0 ± 1.0) good overall ratings and one simulator (Premie HAL S2209: 2.8 ± 1.0) an unfavorable rating.
Conclusion: The simulator physiology deviated significantly from preterm infants' reference values concerning resistance and compliance, potentially promoting a wrong ventilation technique.
Impact: Very low birth weight infant simulators showed physiological properties far deviating from corresponding patient reference values. Only ventilation with very high peak pressure achieved tidal volumes in the simulators, as aimed at in very low birth weight infants, potentially promoting a wrong ventilation technique. Compared to very low birth weight infant cadavers, most tested simulators accurately reproduced the anatomic angular relationships, but their airway dimensions were relatively too large for the represented body. The more professional experience the experts had, the lower they rated the very low birth weight infant simulators.
© 2021. The Author(s).
Conflict of interest statement
P.D. worked as a simulation instructor for SimCharacters (Vienna, Austria) from 2010 to 2013. The remaining authors declare no competing interests.
Figures




References
-
- Johnson L, Mu T, Sawyer T. Use of medical simulation in neonatal-perinatal fellowship training programs. J. Neonatal Perinat. Med. 2012;5:339–345. doi: 10.3233/NPM-1256611. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
