

Integrating HIV services and other health services: A systematic review and meta-analysis
- PMID: 34752477
- PMCID: PMC8577772
- DOI: 10.1371/journal.pmed.1003836
Integrating HIV services and other health services: A systematic review and meta-analysis
Abstract
Background: Integration of HIV services with other health services has been proposed as an important strategy to boost the sustainability of the global HIV response. We conducted a systematic and comprehensive synthesis of the existing scientific evidence on the impact of service integration on the HIV care cascade, health outcomes, and cost-effectiveness.
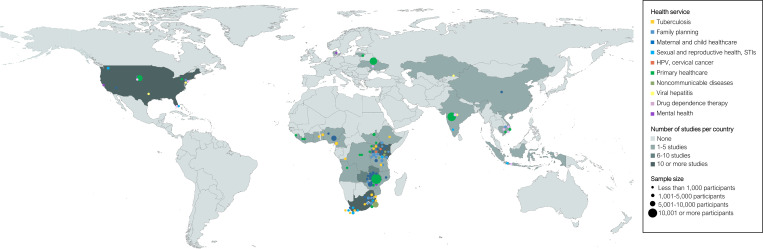
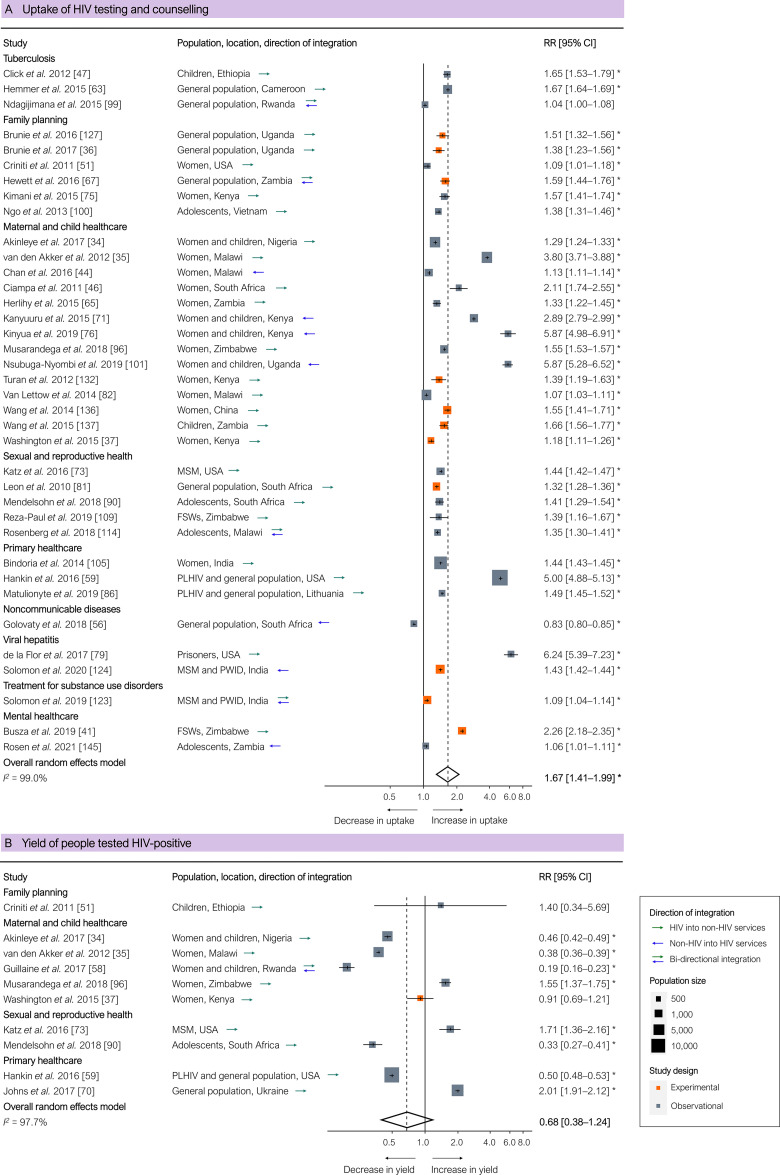
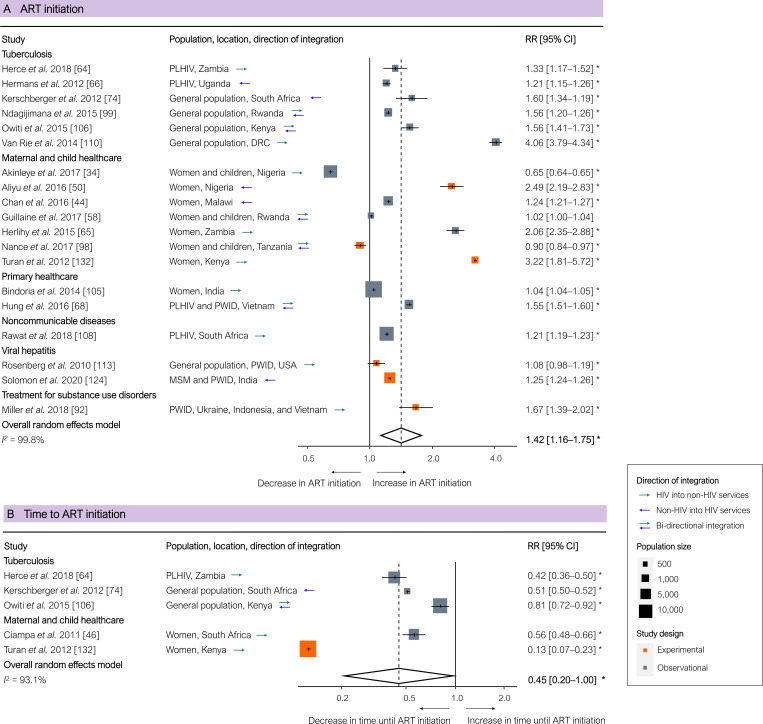
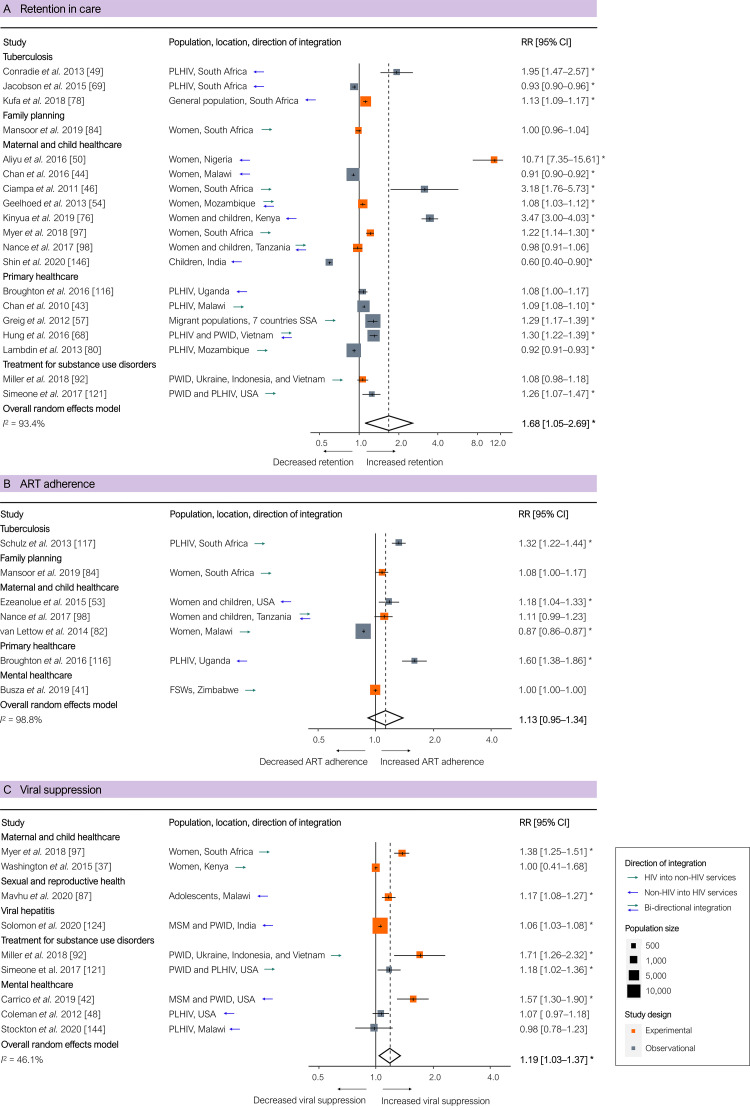
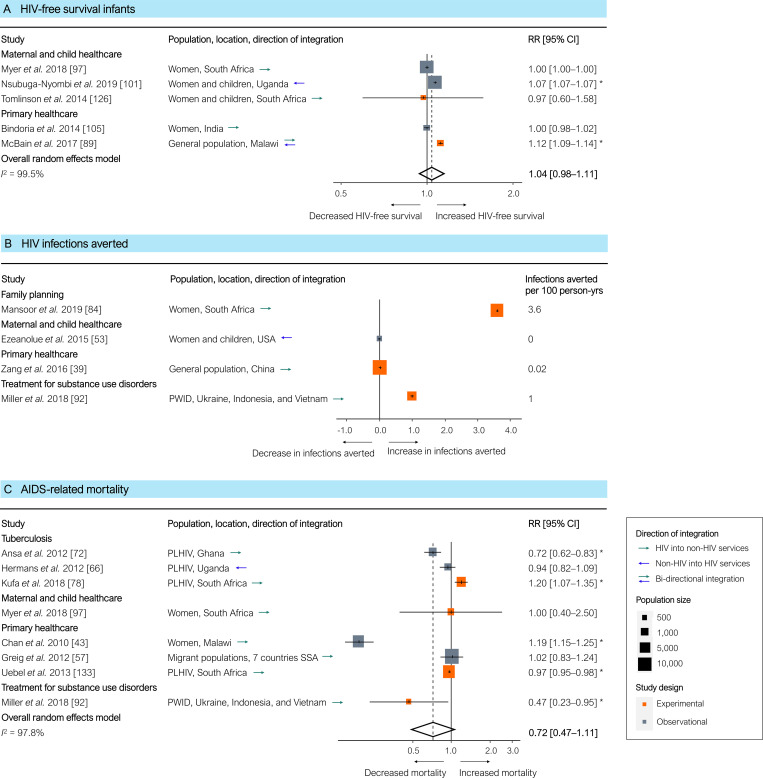
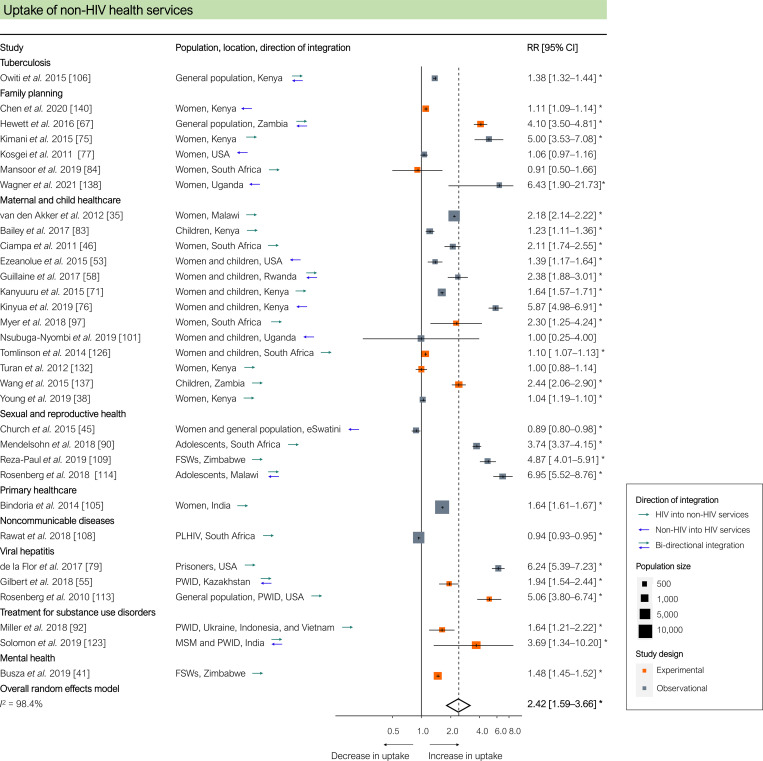
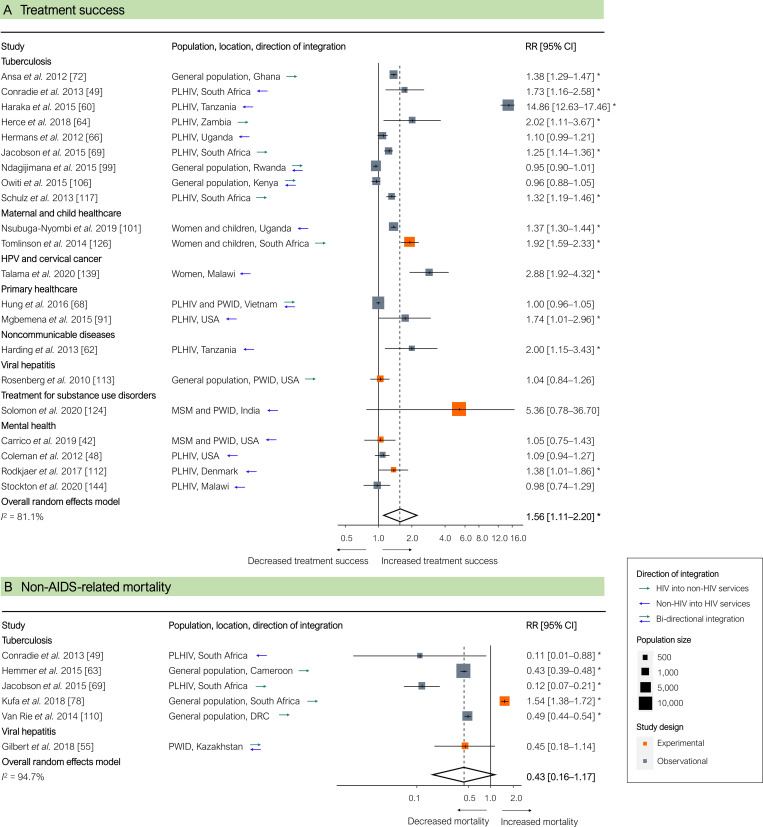
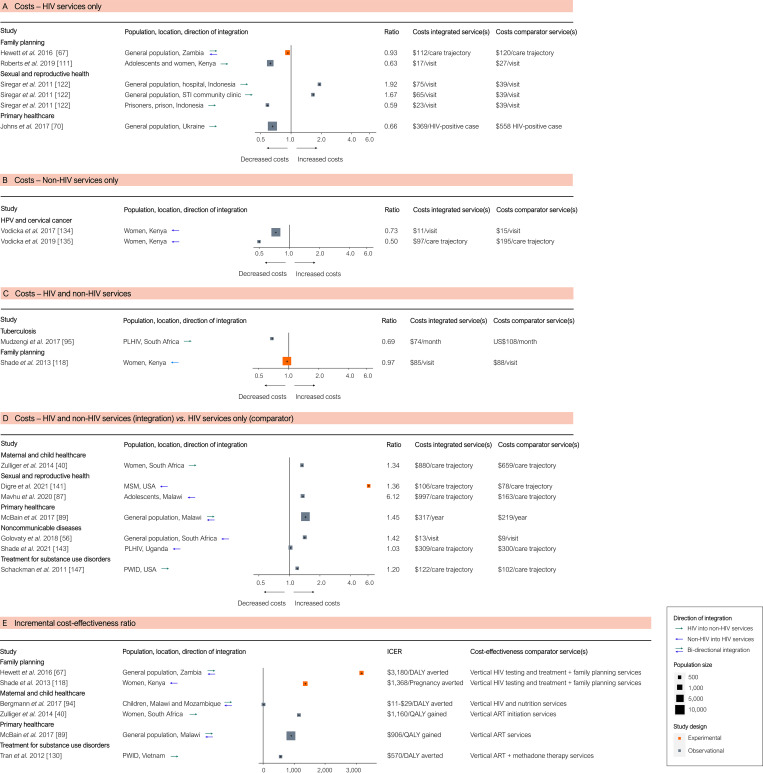
Methods and findings: We reviewed the global quantitative empirical evidence on integration published between 1 January 2010 and 10 September 2021. We included experimental and observational studies that featured both an integration intervention and a comparator in our review. Of the 7,118 unique peer-reviewed English-language studies that our search algorithm identified, 114 met all of our selection criteria for data extraction. Most of the studies (90) were conducted in sub-Saharan Africa, primarily in East Africa (55) and Southern Africa (24). The most common forms of integration were (i) HIV testing and counselling added to non-HIV services and (ii) non-HIV services added to antiretroviral therapy (ART). The most commonly integrated non-HIV services were maternal and child healthcare, tuberculosis testing and treatment, primary healthcare, family planning, and sexual and reproductive health services. Values for HIV care cascade outcomes tended to be better in integrated services: uptake of HIV testing and counselling (pooled risk ratio [RR] across 37 studies: 1.67 [95% CI 1.41-1.99], p < 0.001), ART initiation coverage (pooled RR across 19 studies: 1.42 [95% CI 1.16-1.75], p = 0.002), time until ART initiation (pooled RR across 5 studies: 0.45 [95% CI 0.20-1.00], p = 0.050), retention in HIV care (pooled RR across 19 studies: 1.68 [95% CI 1.05-2.69], p = 0.031), and viral suppression (pooled RR across 9 studies: 1.19 [95% CI 1.03-1.37], p = 0.025). Also, treatment success for non-HIV-related diseases and conditions and the uptake of non-HIV services were commonly higher in integrated services. We did not find any significant differences for the following outcomes in our meta-analyses: HIV testing yield, ART adherence, HIV-free survival among infants, and HIV and non-HIV mortality. We could not conduct meta-analyses for several outcomes (HIV infections averted, costs, and cost-effectiveness), because our systematic review did not identify sufficient poolable studies. Study limitations included possible publication bias of studies with significant or favourable findings and comparatively weak evidence from some world regions and on integration of services for key populations in the HIV response.
Conclusions: Integration of HIV services and other health services tends to improve health and health systems outcomes. Despite some scientific limitations, the global evidence shows that service integration can be a valuable strategy to boost the sustainability of the HIV response and contribute to the goal of 'ending AIDS by 2030', while simultaneously supporting progress towards universal health coverage.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- United Nations. Political declaration on HIV and AIDS: on the fast-track to accelerate the fight against HIV and to end the AIDS epidemic by 2030. New York: United Nations; 2016. doi: 10.1093/oxfordhb/9780199560103.003.0005 - DOI
-
- Joint United Nations Programme on HIV/AIDS. Fast-track—ending the AIDS epidemic by 2030. Geneva: Joint United Nations Programme on HIV/AIDS; 2014. [cited 2021 Oct 13]. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2686_WAD2014rep....
-
- Joint United Nations Programme on HIV/AIDS. UNAIDS 2011–2015 strategy: getting to zero. Geneva: Joint United Nations Programme on HIV/AIDS; 2013. [cited 2021 Oct 13]. Available from: https://www.unaids.org/sites/default/files/media_asset/JC2034_UNAIDS_Str....
-
- Joint United Nations Programme on HIV/AIDS. 90-90-90: an ambitious treatment target to help end the AIDS epidemic. Geneva: Joint United Nations Programme on HIV/AIDS; 2014. [cited 2021 Oct 13]. Available from: https://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf.
-
- Joint United Nations Programme on HIV/AIDS. Seizing the moment: tackling entrenched inequalities to end epidemics—global AIDS update 2020. Geneva: Joint United Nations Programme on HIV/AIDS; 2020. [cited 2021 Oct 13]. Available from: https://www.unaids.org/sites/default/files/media_asset/2020_global-aids-....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
