

Treatment of Delirium During Critical Illness
- PMID: 34752706
- PMCID: PMC9400521
- DOI: 10.1146/annurev-med-042220-013015
Treatment of Delirium During Critical Illness
Abstract
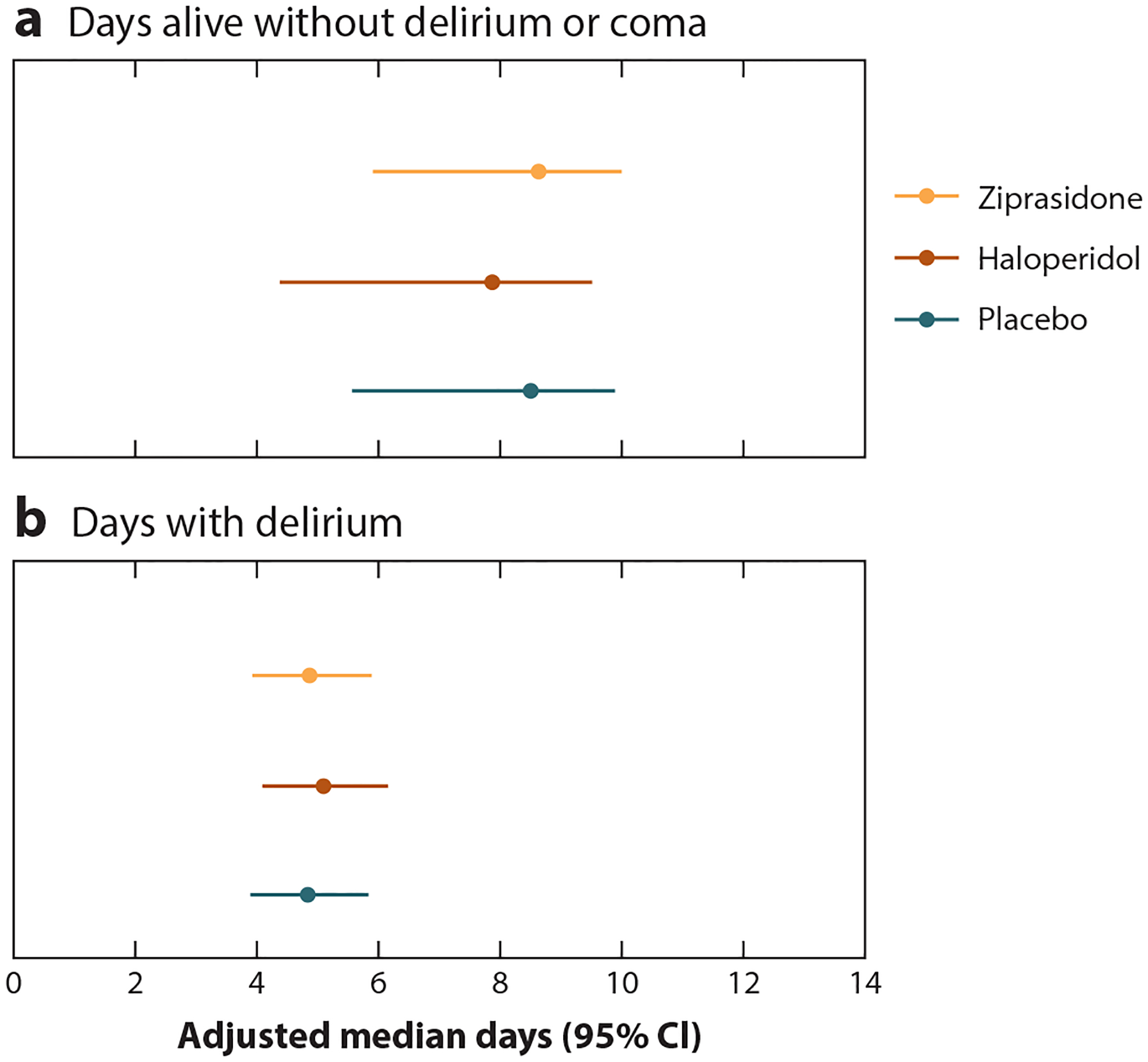
Delirium, an acute disturbance in mental status due to another medical condition, is common and morbid in the intensive care unit. Despite its clear association with multiple common risk factors and important outcomes, including mortality and long-term cognitive impairment, both the ultimate causes of and ideal treatments for delirium remain unclear. Studies suggest that neuroinflammation, hypoxia, alterations in energy metabolism, and imbalances in multiple neurotransmitter pathways contribute to delirium, but commonly used treatments (e.g., antipsychotic medications) target only one or a few of these potential mechanisms and are not supported by evidence of efficacy. At this time, the optimal treatment for delirium during critical illness remains avoidance of risk factors, though ongoing trials may expand on the promise shown by agents such as melatonin and dexmedetomidine.
Keywords: delirium; intensive care; mechanical ventilation; treatment.
Figures


References
-
- Adamis D, Treloar A, Martin FC, Macdonald AJ. 2007. A brief review of the history of delirium as a mental disorder. Hist. Psychiatry 18(72 Pt. 4):459–69 - PubMed
-
- Am. Psychiatr. Assoc. 2013. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. Washington, DC: Am. Psychiatr. Assoc. Publ.
-
- Ely EW, Shintani A, Truman B, et al. 2004. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 291(14):1753–62 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
