

Dose selection and tolerability of anticancer agents evaluated by the European Medicines Agency in the period 2015-2020
- PMID: 34752995
- PMCID: PMC8586755
- DOI: 10.1016/j.esmoop.2021.100301
Dose selection and tolerability of anticancer agents evaluated by the European Medicines Agency in the period 2015-2020
Abstract
Background: Novel anticancer agents are initially evaluated in a palliative setting in phase I studies. The benefit-risk applying the selected dose from these phase I studies can be considered acceptable at time of registration, however, it is unknown if the optimal dose has been selected during drug development.
Methods: The European Medicines Agency (EMA) European Public Assessment Reports (EPARs) overview was used to select anticancer agents evaluated between 2015 and 2020. The dose selection and tolerability data of EMA assessed anticancer agents was analysed to evaluate dose selection.
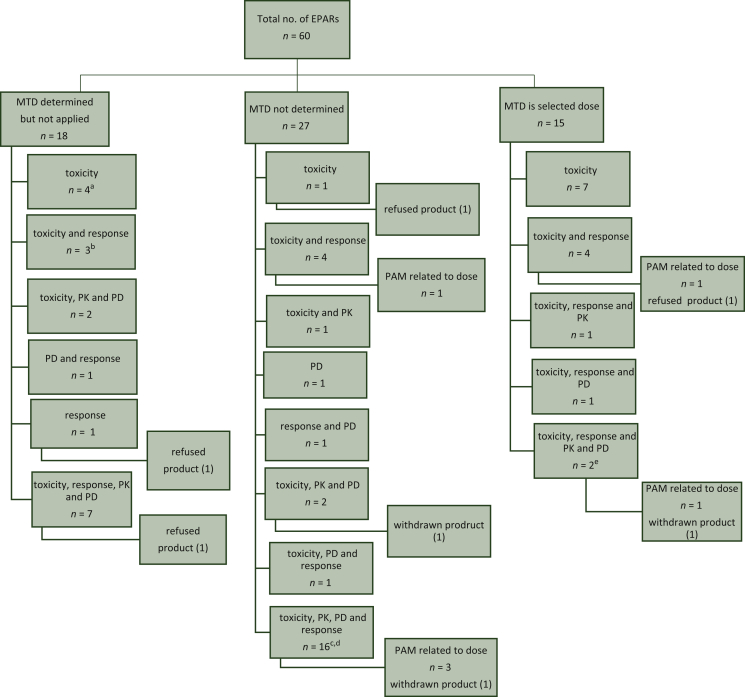
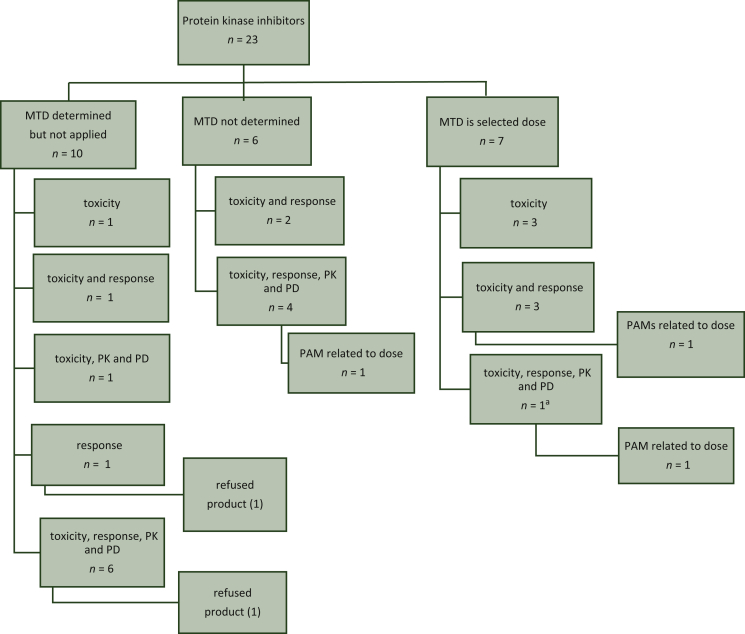
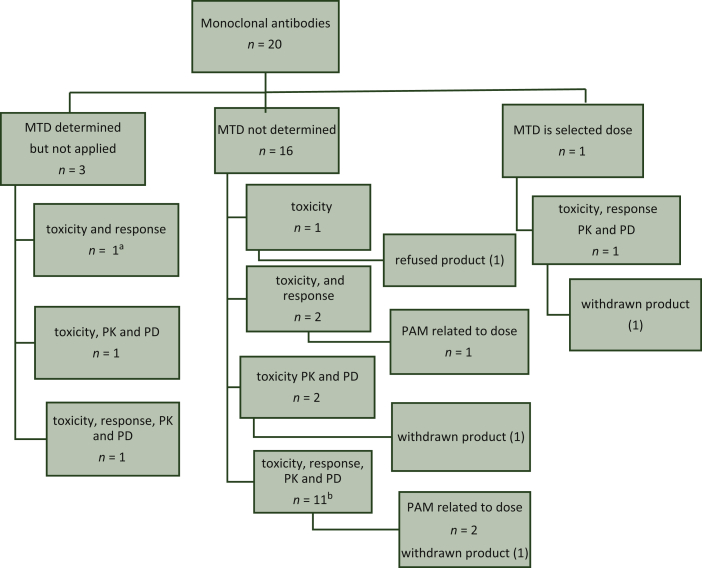
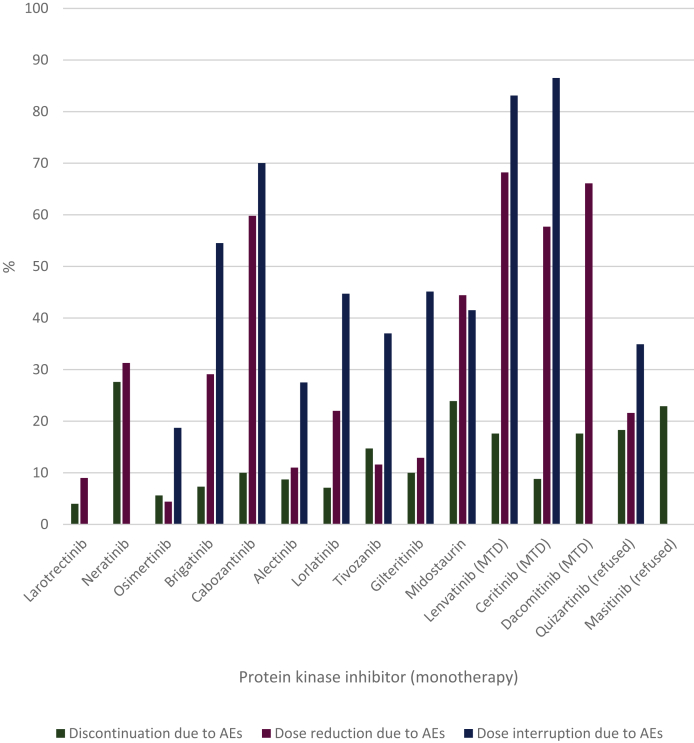
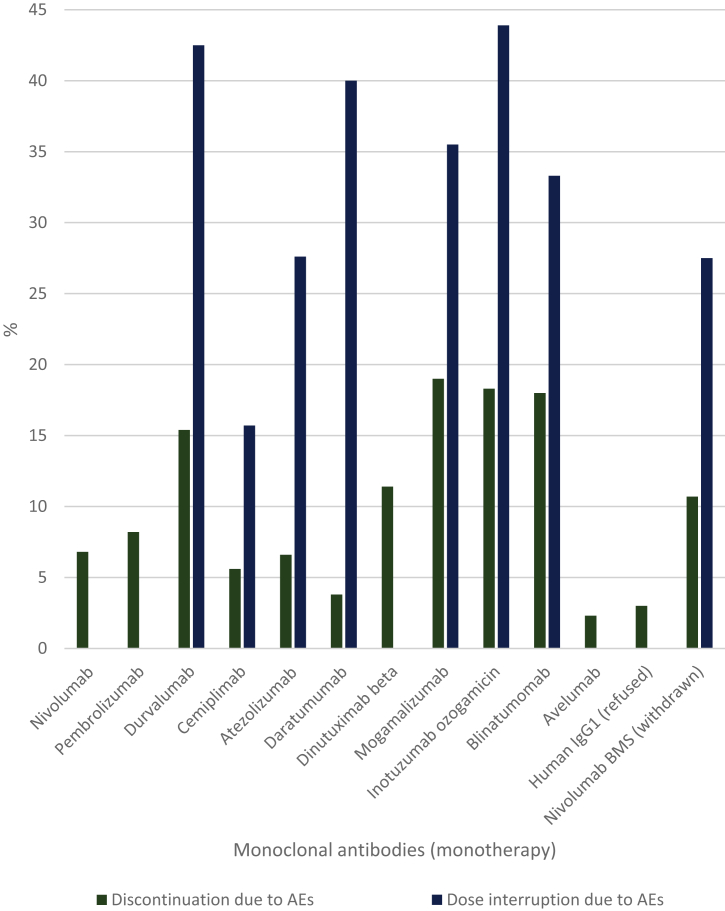
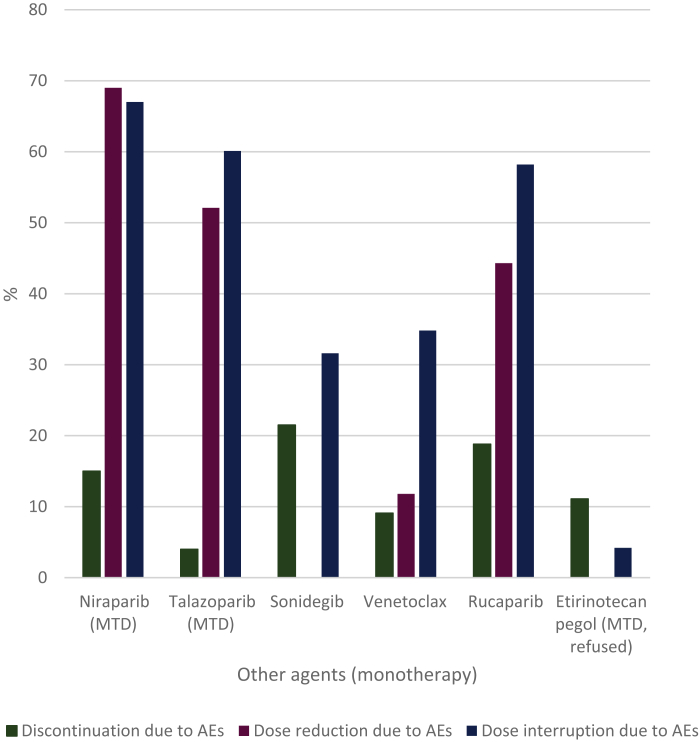
Results: Sixty EPARs were included for analysis. A dose-response relation was identified in five dossiers (8%). The maximum tolerated dose (MTD) was the selected dose for 15 anticancer agents (25%). The MTD was not determined in 27 out of 60 cases (59%). When the MTD was determined but not applied as final dose, the most frequently used dose selection criteria were the combination of toxicity, exposure response, pharmacokinetic data and pharmacodynamic data (in 7 out of 18 cases). Data on tolerability were analysed separately for protein kinase inhibitors and monoclonal antibodies as the dosing interval and mitigation of adverse events (AEs) differs. The median discontinuation, dose reduction and dose interruption rates due to AEs of protein kinase inhibitors were 10%, 26% and 45% for monotherapy and 13%, 47% and 55% for combination therapy, respectively. The median discontinuation rates due to AEs for monoclonal antibodies were 8% for monotherapy and 26% for combination therapy.
Conclusion: The dose-response relationship has not been established for the majority of the registered anticancer agents. The selected posology is often poorly tolerable as reflected by the high discontinuation and dose reduction rates. Due to the absence of dose-response data, it is often unknown if the optimal dose has been selected for anticancer agents.
Keywords: anticancer agents; dose selection; tolerability.
Copyright © 2021 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure The authors have declared no conflicts of interest.
Figures
References
-
- Tenhunen O., Lasch F., Schiel A., Turpeinen M. Single-arm clinical trials as pivotal evidence for cancer drug approval: a retrospective cohort study of centralized European marketing authorizations between 2010 and 2019. Clin Pharmacol Ther. 2020;108(3):653–660. - PubMed
-
- European Medicines Agency (EMA) ICH Topic E4 Dose Response Information to Support Drug Registration. https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e-4-dose... Available at.
-
- Turner D.C., Kondic A.G., Anderson K.M., et al. Pembrolizumab exposure-response assessments challenged by association of cancer cachexia and catabolic clearance. Clin Cancer Res. 2018;24(23):5841–5849. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
