

Utility of preoperative systemic inflammatory biomarkers in predicting postoperative complications after pancreaticoduodenectomy: Literature review and single center experience
- PMID: 34754389
- PMCID: PMC8554715
- DOI: 10.4240/wjgs.v13.i10.1216
Utility of preoperative systemic inflammatory biomarkers in predicting postoperative complications after pancreaticoduodenectomy: Literature review and single center experience
Abstract
Background: The role of preoperative inflammatory biomarkers (PIBs) in predicting postoperative morbidity has been assessed in colorectal and otorhinolaryngeal surgery. However, data regarding the role that preoperative inflammatory biomarkers have on morbidity after pancreaticoduodenectomiy (PD) are less consistent.
Aim: To assess the utility of PIBs in predicting postoperative complications after pancreaticoduodenectomy.
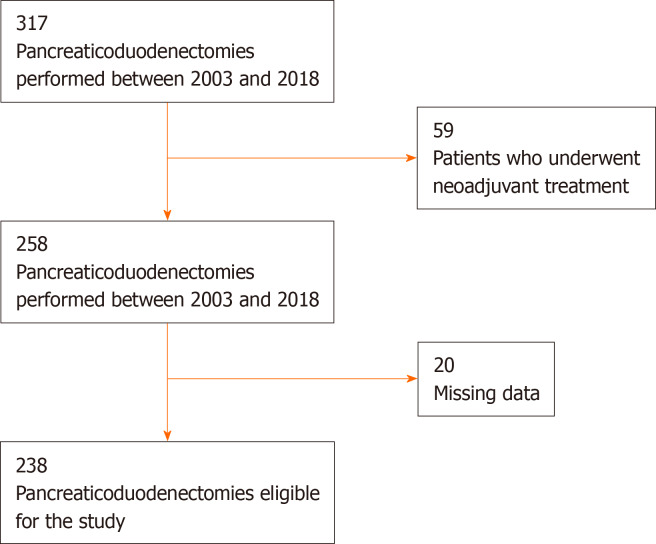
Methods: A database of 317 consecutive pancreaticoduodenectomies performed from April 2003 to November 2018 has been retrospectively analyzed. Data regarding preoperative neutrophil-to-lymphocyte ratio (NLR), derived NLR and C-reactive protein (CRP), and postoperative complications of 238 cases have been evaluated. Exclusion criteria were: age < 18-years-old, previous neoadjuvant treatment, absence of data about PIBs, concomitant hematological disorders, and presence of active infections at the moment of the surgery. PIBs were compared using Mann-Whitney's test and receiver operating characteristic (ROC) analysis was performed to define the cutoffs. The positive predictive value (PPV) was computed to evaluate the probability to develop complication. P-values < 0.05 were considered statistically significant.
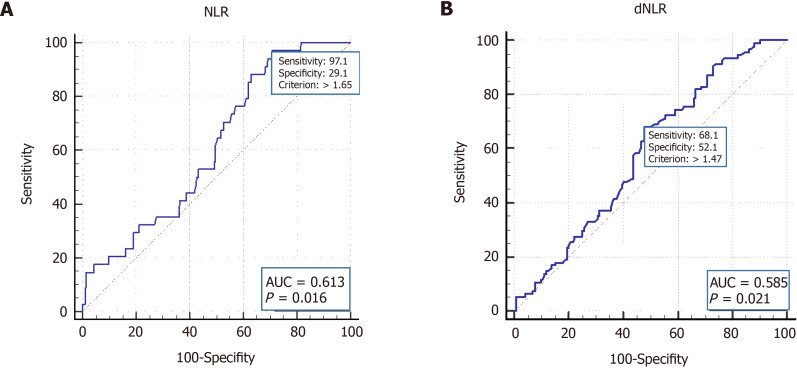
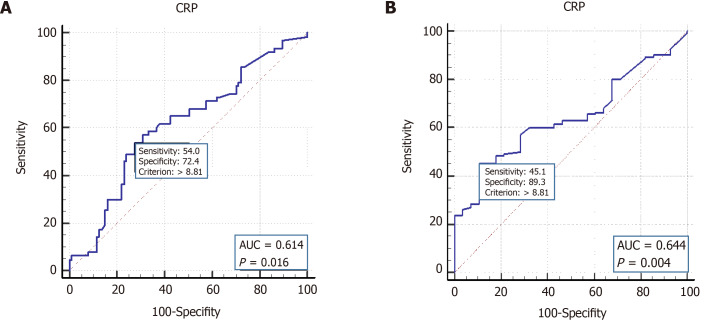
Results: According to the literature findings, only four papers have been published reporting the relation between the inflammatory biomarkers and PD postoperative morbidity. A combination of preoperative and postoperative inflammatory biomarkers in predicting complications after PD and the utility of preoperative NLR in the development of postoperative pancreatic fistula (POPF) have been reported. The combination of PIBs and postoperative day-1 drains amylase has been reported to predict the incidence of POPF. According to our results, CRP values were significantly different between patients who had/did not have postoperative complications and abdominal collections (P < 0.05). Notably, patients with preoperative CRP > 8.81 mg/dL were at higher risk of both overall complications and abdominal collections (respectively P = 0.0037, PPV = 0.95, negative predictive value [NPV] = 0.27 and P = 0.016, PPV = 0.59, NPV = 0.68). Preoperative derived neutrophil-to-lymphocyte ratio (dNLR) (cut off > 1.47) was also a predictor of abdominal collection (P = 0.021, PPV = 0.48, NPV = 0.71). Combining CRP and dNLR, PPV increased to 0.67. NLR (cut off > 1.65) was significantly associated with postoperative hemorrhage (P = 0.016, PPV = 0.17, NPV = 0.98).
Conclusion: PIBs may predict complications after PD. During postoperative care, PIB levels could influence decisions regarding the timing of drains removal and the selection of patients who might benefit from second level diagnostic exams.
Keywords: Complications; Derived neutrophil-to-lymphocyte ratio; Neutrophil-to-lymphocyte ratio; Pancreaticoduodenectomy; Preoperative inflammatory markers.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All authors declare that they do not have any conflict of interest.
Figures
References
-
- Kamarajah SK. Pancreaticoduodenectomy for periampullary tumours: a review article based on Surveillance, End Results and Epidemiology (SEER) database. Clin Transl Oncol. 2018;20:1153–1160. - PubMed
-
- Giuliano K, Ejaz A, He J. Technical aspects of pancreaticoduodenectomy and their outcomes. Chin Clin Oncol. 2017;6:64. - PubMed
-
- Caputo D, Angeletti S, Ciccozzi M, Cartillone M, Cascone C, La Vaccara V, Coppola A, Coppola R. Role of drain amylase levels assay and routinary postoperative day 3 abdominal CT scan in prevention of complications and management of surgical drains after pancreaticoduodenectomy. Updates Surg. 2020;72:727–741. - PubMed
-
- Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, Allen P, Andersson R, Asbun HJ, Besselink MG, Conlon K, Del Chiaro M, Falconi M, Fernandez-Cruz L, Fernandez-Del Castillo C, Fingerhut A, Friess H, Gouma DJ, Hackert T, Izbicki J, Lillemoe KD, Neoptolemos JP, Olah A, Schulick R, Shrikhande SV, Takada T, Takaori K, Traverso W, Vollmer CR, Wolfgang CL, Yeo CJ, Salvia R, Buchler M International Study Group on Pancreatic Surgery (ISGPS) The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery. 2017;161:584–591. - PubMed
-
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, Neoptolemos JP, Padbury RT, Sarr MG, Traverso LW, Yeo CJ, Büchler MW. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS) Surgery. 2007;142:761–768. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
